

The benefits of couple and family therapy are clear: systemic interventions are generally effective at increasing relationship satisfaction, improving communication, bolstering individual mental health, and reducing problematic behaviors (Wittenborn & Holtrop, 2021).
But not every client leaves therapy with the improvement they hope for. Surprisingly, a substantial number of clients get worse over the course of therapy. For example, one study of treated couples found that 30-60% experienced deterioration rather than improvement (Snyder et al., 2006).
How good are therapists at predicting which clients will get better and which will get worse? Sadly, not very good.
Research in individual therapy has shown that therapists are no better than chance at predicting client deterioration (Hatfield et al., 2009). While there is no research on systemic therapists, we have no reason, beyond our bias, to suspect that they would be any different.
This blind spot poses a significant practical and ethical issue. How do we intervene and change the course of treatment when our clients start to deteriorate if we don’t know that it’s happening? Furthermore, the AAMFT Code of Ethics states that it is only ethical for marriage and family therapists (MFTs) to continue therapeutic relationships “so long as it is reasonably clear that clients are benefitting from the relationship” (AAMFT, 2026). If we are no better than chance at knowing whether our clients are going to deteriorate, how can we know they are benefiting from the therapeutic relationship?
Clearly, MFTs would benefit from an increased capability to predict and detect client change. Where can we turn for a solution? The answer may be simpler than you think.
Using “best science”
Evidence-based practice provides an important formula for therapeutic effectiveness (APA, 2006):
Best Science + Clinical Experience & Intuition + Patient Characteristics/Preferences/Culture
As trained systemic thinkers, MFTs are likely proficient at using clinical intuition and valuing contextual factors at each level of the client system. But what about using the “best science”?
Measurement-based care
One approach to using “best science” in therapy is by implementing measurement-based care (MBC). MBC is a clinical process that involves routinely administering client-reported outcome measures throughout treatment, using the information to inform assessment and to initiate discussions with clients about their progress. Therapists can then modify treatment based on these discussions. In short, it’s a scientifically backed method of answering, “Is the treatment I’m providing working for this client?”
Let’s look at an example of how MBC works. Ana and Mateo are pursuing couple therapy to reduce conflict and have more open communication. At intake, Ana and Mateo complete several measures selected by the therapist to give an accurate picture of their needs and goals. The therapist may introduce these measures by saying something like this:
Therapist: Ana and Mateo, thank you so much for taking the time to complete the questionnaires I sent you before our session. I know that took some time out of your day to do. Before each of our sessions together, you’ll be asked to complete a few of them again. The reason I do this is to allow you to have a voice in your treatment. Using these assessments, I can understand your needs and track your progress so we can be sure that therapy is helpful for you. I’ll be keeping track of your responses to these assessments and in the future, I may bring up patterns or changes I notice so that we can discuss how therapy can be more beneficial to you. Do you have any questions about this?
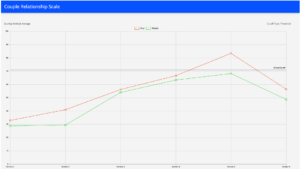
Before every subsequent session, Ana and Mateo are emailed a link to fill out a few measures again, which take one to two minutes to complete. The therapist can track their progress on these measures, using a regularly updated graph like the example below.


One of the measures the therapist chooses to use assesses the clients’ perceptions of the therapeutic alliance. Over the first four sessions, the therapist observes a steady increase in Ana and Mateo’s perceptions of the alliance. However, in the fifth session, the therapist intervenes in a way that leaves Ana feeling uncomfortable. Ana conceals her discomfort, and the therapist moves on without realizing the true impact of the intervention. It isn’t until next session, when the therapist views the results of Ana’s assessments, that she notices a steep drop in Ana’s perception of the alliance.
Using this information, the therapist can gently address this drop next session. This interaction might look something like this:
Therapist: Thank you again for completing those questionnaires before our session! I’d like to take a few minutes to discuss some of your responses. Is that okay?
Ana & Mateo: Sure.
Therapist: Ana, I noticed that you rated how much I care about you much lower this time than in the past. That signaled to me that something may have happened last session that made you feel uncomfortable or unsafe with me. Am I on the right track?
Ana: (visibly nervous) Yeah.
Therapist: I’m so grateful you answered honestly on the questionnaire. It’s really brave of you to be authentic about your experience in therapy, and this allows us to talk about what happened and get back on the same page. I want to take full accountability for what I did that made you feel this way—even if I didn’t realize it. I care about how you feel, and it’s important to me that you feel safe here.
Ana: (appears more at ease) Thank you.
Therapist: So, let’s talk about it. Can you share with me what happened and how it made you feel?
Ana: Yeah. I guess it was when you said…
Instead of continuing a course of treatment that wasn’t working for Ana, the therapist used Ana’s responses to discuss her needs and alter treatment to better meet them. If the therapist had chosen not to implement MBC in her practice, she may have never noticed this alliance rupture. In the worst-case scenario, Ana and Mateo may have dropped out of treatment or continued without experiencing improvement.
This is just one example of the countless ways MBC can be implemented to predict client outcomes and improve treatment. How many times have you had a couple or family present to therapy appearing distant and off, only to deny that anything is wrong until the last five minutes of the session, when they reveal they had the biggest argument ever that week? Routinely measuring outcomes such as relationship satisfaction allows MFTs to detect changes in symptoms as soon as they occur, guide treatment to address what clients need, and avoid wasting session time. For example:
Therapist: It’s so good to see you both. Let’s begin by talking about your responses to the relationship satisfaction measure you completed today. Mateo, your sense of trust in Ana plummeted from a nine out of 10 to a two out of 10 this week. And Ana, you reported that the two of you have been arguing much more than usual. Clearly, something big happened since the last time I saw you. Let’s start there.
Couple therapists may monitor their couple clients’ progress on regularly updated graphs such as this one:

Rather than relying on chance to predict which clients are benefiting from therapy and which are getting worse, by using MBC, you can be confidently informed of your clients’ progress and regularly adjust treatment to target their needs.
Benefits of measurement-based care
Using MBC improves the effectiveness of treatment and reduces clients’ risk of deterioration by 33% (Miller et al., 2015). Particularly, at-risk clients may benefit the most. There are varied definitions of “at-risk” clients, but generally, they discuss clients who don’t follow typical change trajectories or who have issues of safety, such as violence and suicide ideation. Additionally, clients who present with concurrent problems are “largely disadvantaged” when compared to clients with one problem (Scott & Gorey, 2025; p. 251). Research shows that routinely monitoring outcomes allows therapists to monitor suicidal ideation, violence, and other safety issues closely (Tilden & Wampold, 2017). Further, MBC is particularly helpful for clients who are not on track (Barkham et al., 2023). MBC helps those most at risk of treatment failure (McAleavey et al., 2024).
Using MBC to accurately target clients’ needs may shorten treatment, thereby driving down the cost of care (Miller et al., 2015). MBC also gives clients a greater voice in their own treatment, facilitating communication and collaboration between clients and therapists (APA, n.d.). Reporting on their perceived outcomes each session allows clients to increase their awareness of inner states and feelings and may lead to greater respect for their therapist because it communicates that their voice is valued (APA, n.d.).
Systemic therapy may see unique benefits, including a decreased risk of separation and divorce for couples being treated with MBC compared to couples in treatment-as-usual (Anker et al., 2009). Using MBC with couples may also lead to improved psychological functioning and relationship outcomes. In fact, one study found that four times more couples experienced recovery when their therapists used MBC compared to treatment-as-usual (Reese et al., 2010).
MBC also benefits therapists and supervisors. MBC reduces dropout (de Jong et al., 2021) and improves therapeutic alliance (Brattland et al., 2019). It provides a lot of information about clients before the session begins, alerting therapists to critical issues and offering them time to prepare to address them. Perhaps most importantly, MBC allows therapists to identify clients who are deteriorating so that necessary course corrections can be made in treatment (de Jong et al., 2021). Lastly, it improves objectivity in supervision and gives supervisors a reliable way to track the progress of their supervisees’ clients.
Common Concerns
The benefits of MBC for clients, therapists, supervisors, and the therapeutic process are clear. But some readers may still be skeptical. Below, we address some common myths about using MBC:
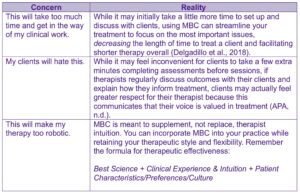

While using MBC may involve minor inconvenience at first, any cons are far outweighed by the long-term benefits it will offer you and your clients.
Getting started
We strongly encourage all MFTs to implement this resource into their practice, and doing so is quite simple. Many electronic health record (EHR) systems, such as Clerie, Greenspace Mental Health, SimplePractice and TherapyNotes, now have built-in tools for monitoring client outcomes. Beyond EHRs, several web-based tools have been developed to track client outcomes. For example, the Partners for Change Outcome Management System (PCOMS; Duncan & Reese, 2015) is geared towards individual therapy outcomes. There are also tools specifically tailored to couple and family therapy, including the Systemic Therapy Inventory of Change (STIC; He et al., 2019), SYPRENE (Vitry et al., 2020), and the Marriage and Family Therapy Practice Research Network (MFT-PRN; Johnson et al., 2017).
For more information about how to get started with MBC, visit the Yale Measurement Based Care Collaborative.
Conclusion
In their review of MBC in couple and family therapy, Lappan et al. (2018) said the following: “It is crucial and ethical for couple and family therapists to use formalized feedback mechanisms as a standard part of their clinical work.” As therapists, we may be no better than chance at predicting change on our own, but by implementing “best science” in our practice, we can strengthen our detection of client deterioration, greatly improve client outcomes, and become more ethical and effective clinicians overall.


Julia Christensen, MS, AMFT, is an AAMFT Student member and a PhD student of Marriage and Family Therapy at Brigham Young University. She is an associate marriage and family therapist working towards full licensure and supervisory certification. Her research and clinical work focus on strengthening couple relationships with significant value, belief, and/or ideological differences.

Shayne Anderson, PhD, LMFT, is an AAMFT Professional member holding the Approved Supervisor and Clinical Fellow designations, and Professor of Marriage and Family Therapy at Brigham Young University. He is passionate about couple therapy process research and has authored several professional presentations on the benefits of measurement-based care for MFTs and their clients. He is the co-developer of the Marriage and Family Therapy Practice Research Network (MFT-PRN), a free online tool used to facilitate measurement-based care for clients at participating clinics.

Daniel Frost, PhD, is the director of public scholarship in the School of Family Life at Brigham Young University. He also serves as editor-in-chief of Public Square Magazine.

Lee Johnson, PhD, LMFT, is an AAMFT Professional member holding the Approved Supervisor and Clinical Fellow designations, and Professor of Marriage and Family Therapy at Brigham Young University. His research focuses on emotion regulation and couple and family relationships in clinical settings, particularly how physical exercise, sleep, and stress relate to therapy processes and outcomes. He is the co-developer of the Marriage and Family Therapy Practice Research Network (MFT-PRN).
American Association for Marriage and Family Therapy. (2026). Code of ethics. https://www.aamft.org/AAMFT/Legal_Ethics/Code_of_Ethics.aspx
American Psychological Association. (n.d.). Measurement-based care. APA Services. Retrieved January 31, 2026, from https://www.apaservices.org/practice/measurement-based-care
Anker, M. G., Duncan, B. L., & Sparks, J. A. (2009). Using client feedback to improve couple therapy outcomes: A randomized clinical trial in a naturalistic setting. Journal of Consulting and Clinical Psychology, 77, 693–704.
APA Presidential Task Force on Evidence-Based Practice (2006). Evidence-based practice in psychology. The American psychologist, 61(4), 271–285. https://doi.org/10.1037/0003-066X.61.4.271
Barkham, M., De Jong, K., Delgadillo, J., & Lutz, W. (2023). Routine outcome monitoring (ROM) and feedback: Research review and recommendations. Psychotherapy Research, 33(7), 841–55. https://doi.org/10.1080/10503307.2023.2181114.
Brattland, H., Koksvik, J. M., Burkeland, O., Klöckner, C. A., Lara-Cabrera, M. L., Miller, S. D., Wampold, B., Ryum, T., & Iversen, V. C. (2019). Does the working alliance mediate the effect of routine outcome monitoring (ROM) and alliance feedback on psychotherapy outcomes? A secondary analysis from a randomized clinical trial. Journal of Counseling Psychology, 66(2), 234-246. https://doi.org/10.1037/cou0000320
de Jong, K., Conijn, J. M., Gallagher, R. A. V., Reshetnikova, A. S., Heij, M., & Lutz, M. C. (2021). Using progress feedback to improve outcomes and reduce drop-out, treatment duration, and deterioration: A multilevel meta-analysis. Clinical Psychology Review, 85. https://doi.org/10.1016/j.cpr.2021.102002
Delgadillo J, Overend K, Lucock M, Groom M, Kirby N, McMillan D, Gilbody S, Lutz W, Rubel JA, de Jong K. (2017). Improving the efficiency of psychological treatment using outcome feedback technology. Behaviour Research and Therapy, 99:89–97.
Duncan, B. L., & Reese, R. J. (2015). The Partners for Change Outcome Management System (PCOMS) revisiting the client’s frame of reference. Psychotherapy (Chicago, Ill.), 52(4), 391–401. https://doi.org/10.1037/pst0000026
Hatfield, D., McCullough, L., Frantz, S., & Krieger, K. (2009). Do we know when our clients get worse? An investigation of therapists’ ability to detect negative client change. Clinical Psychology & Psychotherapy. https://doi.org/10.1002/cpp.656
He, Y., Hardy, N. R., Zinbarg, R. E., Goldsmith, J. Z., Kramer, A., Williams, A. L., & Pinsof, W. M. (2019). The Systemic Therapy Inventory of Change (STIC) Initial Scales: Are they sensitive to change?. Psychological assessment, 31(9), 1107–1117. https://doi.org/10.1037/pas0000729
Johnson, L. N., Miller, R. B., Bradford, A. B., & Anderson, S. R. (2017). The Marriage and Family Therapy Practice Research Network (MFT-PRN): Creating a More Perfect Union Between Practice and Research. Journal of marital and family therapy, 43(4), 561–572. https://doi.org/10.1111/jmft.12238
Lappan, S., Shamoon, Z., & Blow, A. (2018). The importance of adoption of formal client feedback in therapy: A narrative review. Journal of Family Therapy, 40(4), 466–488. https://doi-org.byu.idm.oclc.org/10.1111/1467-6427.12183
McAleavey, A. A., De Jong, K., Nissen-Lie, H. A., Boswell, J. F., Moltu, C., & Lutz, W. (2024). Routine outcome monitoring and clinical feedback in psychotherapy: Recent advances and future directions. Administration and Policy in Mental Health and Mental Health Services Research, 51(3), 291–305. https://doi.org/10.1007/s10488-024-01351-9.
Miller, S. D., Hubble, M. A., Chow, D., & Seidel, J. (2015). Beyond measures and monitoring: Realizing the potential of feedback-informed treatment. Psychotherapy, 52(4), 449–457. https://doi.org/10.1037/pst0000031
Reese, R. J., Toland, M. D., & Slone, N. C. (2010). Effect of client feedback on couple psychotherapy outcomes. Psychotherapy Theory, Research, Practice, Training, 47, 616–630. https://doi.org/10.1037/a0021182
Scott, K. D. & Gorey, K. M. (2025). Concurrent disorders and treatment outcomes: A meta-analysis. Journal of Dual Diagnosis, 21(3), 251–65. https://doi.org/10.1080/15504263.2025.2515015.
Snyder, D. K., Castellani, A. M., & Whisman, M. A. (2006). Current status and future directions in couple therapy. Annual review of psychology, 57, 317–344. https://doi.org/10.1146/annurev.psych.56.091103.070154
Tilden, T. & Wampold, B. E., (2017). Routine outcome monitoring in couple and family therapy: The empirically informed therapist. Springer International Publishing, https://doi.org/10.1007/978-3-319-50675-3.
Vitry, G., Duriez, N., Lartilleux-Suberville, S., Pakrosnis, R., Beau, A., Garcia-Rivera, T., Brosseau, O., Vargas Avalos, P., Bardot, E. and Ray, W.A. (2020), Introducing SYPRENE: An international practice research network for strategic and systemic therapists and researchers. Family Process, 59: 1946-1957. https://doi.org/10.1111/famp.12520
Wittenborn, A. K., & Holtrop, K. (2022). Introduction to the special issue on the efficacy and effectiveness of couple and family interventions: Evidence base update 2010-2019. Journal of marital and family therapy, 48(1), 5–22. https://doi.org/10.1111/jmft.12576
Other articles


Being a Positive Advocate When an Elder Needs Hospital Care
A large part of my work with caregivers has involved helping them learn how to be effective advocates when an elder requires hospital care. Advocacy refers to the actions you take to support the elder so they receive the best possible care and outcomes.
Nancy L. Kriseman, MSW

When the World Becomes Too Much: Living in Oscillanguish
There are moments in history when the emotional life of individuals cannot be understood outside of the systems they are embedded in. Moments when distress is not simply internal, but relational, political, technological, and collective.
Afarin Rajaei, PhD

Sleep Problems Are Relationship Problems: Why MFTs Should Be Leading Dyadic Sleep Interventions
Marriage and family therapists (MFTs) know something that sleep medicine has taken decades to discover: human problems don’t exist in isolation. When someone can’t sleep, it’s rarely just their problem. It’s a couple problem. A family problem. A relationship problem.
Bruce D. Forman, PhD