

A Beginner’s Guide for Mental Health Professionals and Allied Fields
Affecting millions of people worldwide, migraine is considered one of the top 10 most disabling medical conditions by the World Health Organization (WHO). The condition has an estimated worldwide prevalence of 15-18% (Khan et al., 2021), including over 37 million Americans (American Migraine Foundation, n.d.; Walter, 2022). Migraine is a serious and debilitating medical condition characterized by significant throbbing head pain that is accompanied by various sensory, motor, and somatosensory disturbances. These symptoms not only lead to significant functional impairments in family, social, education, and employment settings, but also frequently co-occur with psychiatric symptoms. As such, mental health professionals can help ensure clients with migraine are accurately assessed and referred for appropriate diagnostic and treatment services. This article aims to increase awareness of migraine in mental health settings through a brief review of the condition, comorbidity with psychiatric symptoms, screening and assessment opportunities, available interventions, and an illustrative case study.
Migraine: Symptoms, causes, phases, and subtypes
Migraine is typified by throbbing head pain, nausea, vomiting, and sensitivity to light and sound (i.e., photophobia and phonophobia, respectively). This can be experienced in one half of the head (i.e., unilateral headache), but it is not uncommon for migraine sufferers to experience pain on both sides of the head simultaneously (i.e., bilateral pain). Physical movement often exacerbates the negative experiences of this disorder (Khan et al., 2021). Considered a chronic condition for many, migraine episodes typically last from 4 hours up to 72 hours (Walter, 2022).
Although the causes of migraine are not fully understood, research suggests this condition results from a complex interaction of many factors. Potential contributors include neurological causes (e.g., neurochemical imbalances, genetics, and hormonal factors, inflammatory mediators, neuropeptides, serotonin pathways, gut microbiota), environmental factors (e.g., weather changes, sensory stimuli such as bright lights, air quality, odors, and loud noises), and lifestyle factors (e.g., sleep, diet, hydration, and exercise; Friedman & De Ver Dye; 2009).
Migraine sufferers often express gastrointestinal (GI) symptoms and autonomic symptoms. Also, researchers have observed a higher prevalence of headaches in patients with GI complaints (Martami et al., 2018), and those patients suffering from inflammatory bowel disease and celiac disease often suffer from migraines (Dimitrova et al., 2013). Current evidence also indicates an association between migraines and other GI disorders, including Helicobacter pylori (H. pylori) infection and irritable bowel syndrome (IBS; Arzani et al., 2020). While the true mechanism of the relationship between GI disorders and migraine is not fully elucidated, one underlying explanation is ascribed to an increase in gut permeability (i.e., leaky gut) and inflammatory responses (van Hemert et al., 2014). There is a bidirectional relationship between gut permeability and inflammation, as studies have shown that an increase in gut permeability can trigger inflammation, and inflammation can cause an increase in gut permeability (Marchiando et al., 2010). This interrelationship appears to be influenced by multiple factors, including inflammatory mediators, gut microbiota composition, neuropeptides, stress hormones, and nutritional compounds (Arzani et al., 2020).

A leaky gut can let harmful substances like lipopolysaccharides, molecules from bacteria, pass from the intestines into the bloodstream. This can trigger a strong immune response and lead to the release of pro-inflammatory cytokines, which are proteins that help the body respond to threats (Menningen & Brewer, 2009; Martami et al., 2019). Many studies have shown that the over-production of these pro-inflammatory cytokines interact with the nociceptors which are part of the chemosensory system of the trigeminal nerve causing increased levels of vasoactive neuropeptides which can contribute to neurogenic inflammation and trigger migraine (Martami et al., 2019). Further, through recent research, the relationship between the immune system and the gut microbiota is becoming clearer. In people with migraines, gut symptoms during attacks have been linked to imbalances in the gut microbiome (Chen et al., 2020; Zhou et al., 2024).
As stated above, migraine sufferers may also exhibit autonomic symptoms that are particularly relevant to mental health providers, including comorbid conditions such as depression, anxiety, and chronic stress (Khan et al., 2021). Typically, clients with migraine present with a combination of these factors. For instance, a person might only experience migraines when exposed to bright lights during (a) hormonal fluctuations and (b) periods of high stress.
The experience of migraine occurs in phases. The throbbing pain, light sensitivity, and sound sensitivity take place in four distinct but often overlapping phases: the prodromal, aura, headache, and post-dromal phases (Khan et al., 2021; Shabani & Ghari Saadati, 2019; NIH, 2025). An overview of the phases of migraine is provided below. How a person experiences these phases can be classified into subtypes (NIH, 2025).
The four phases of migraine:
Prodromal
- Preceding a migraine, prodromal symptoms begin up to 72 hours before the headache phase.
- Symptoms include fatigue, food cravings, phonophobia, mood swings, and neck stiffness.
Aura
- Only about a third of migraine patients experience the aura phase.
- Includes visual disturbances, sensory changes, auditory changes, and speech and language issues.
Headache
- Unilateral or bilateral throbbing or pulsating pain.
- May be moderate or severe in intensity.
Post-dromal
- Intracranial activation of the hypothalamus and thalamus.
- Results in mood swings, food cravings, phonophobia, and irritability.
Types of migraine:
Migraine with typical aura
- Vision changes, sensory changes, and difficulty speaking.
Migraine with brainstem aura
- At least two symptoms of the following: vertigo, double vision, poor muscle coordination, slurred speech, ringing in the ears, hearing loss, and fainting.
Hemiplegic migraine
- Temporary paralysis before or during headache on one side of the body.
- Rare and genetic in origin.
Retinal migraine
- Vision changes, including temporary vision loss.
Chronic migraine
- Over a 3-month period, the patient experiences headaches on at least 15 days in each month.
Menstrual migraine
- People who menstruate experience headaches 2 out of 3 cycles at the onset of their cycle.
Understanding comorbidity between migraine and psychological disorders

Research has found significant comorbidity between migraine and psychiatric disorders (for an overview, see see below; Anderson, 2019; Balaban et al., 2012). This relationship is bidirectional in nature (McCracken et al., 2024). On one hand, the presence of psychiatric comorbidities can cause and exacerbate the frequency and severity of migraine attacks. On the other hand, migraine can contribute to conditions such as anxiety, depression, and stress-related disorders.
The comorbidity of migraine, and multiple psychiatric disorders such as major depressive disorder, general anxiety disorder, and eating disorders have important clinical implications (Badaeva et al., 2023). Foremost, individuals with both migraine and mental health disorders often experience great disability and lower quality of life compared to those with only one of these conditions. As such, individuals who suffer from any of these problems should be screened for all of them. Greater understanding of the shared vulnerabilities between these conditions can facilitate a comprehensive approach to migraine management and improved quality of life for clients (Dindo et al., 2017).
Common psychological disorders comorbid with migraine:
Major Depressive Disorder (MDD)
- Individuals with migraine are 2-4 times more likely to experience depression.
- Comorbidity is linked to increased migraine frequency, severity, and reduced treatment efficacy.
Generalized Anxiety Disorder (GAD)
- Over 50% of migraine sufferers meet the criteria for at least one anxiety disorder, contributing to increased migraine frequency and disability.
Attention-Deficit/Hyperactivity Disorder (ADHD)
- ADHD frequently co-occurs with migraine, exacerbating migraine severity and disability.
Bipolar Disorder
- Higher prevalence in migraine individuals, particularly type II; complicates treatment strategies due to mood instability.
Eating Disorders
- Commonly present in individuals with migraine.
Post-Traumatic Stress Disorder (PTSD)
- The history of trauma (particularly during childhood) is notably more common in chronic migraine sufferers; linked to increased migraine frequency.
Obsessive-Compulsive Disorder (OCD)
- Identified as a comorbid condition in individuals with migraine that potentially exacerbates migraine symptoms.
Sleep-Wake Disorders
- Sleep disturbances, including insomnia, are common in people experiencing migraine and can exacerbate migraine frequency and severity (Merrill, 2023).
Substance Use Disorders
- Higher rates of substance use problems are observed in individuals with chronic migraine (Lipton, 2020).
Screening for Migraine: Recognizing red flags for medical referral and mental health treatment
Clinicians are uniquely positioned to catch critical warning signs for migraine that may otherwise go undetected. Although not qualified to diagnose migraine or other related disorders, mental health professionals are often one of the first points of contact for individuals struggling with mental distress and chronic pain, such as migraine. The incorporation of migraine screening into mental health assessments can facilitate the early identification of symptoms and referrals to appropriate medical providers. There are several easy-to-use screening instruments for migraine, which mental health professionals can research and access online. However, additional training, education, and consultation are needed before implementing such practices into the work of mental health providers. Mental health professionals need to ensure that they are working within their scope of competency and in compliance with their respective boards. Below are a handful of common screening tools. The results from these tools can help provide a comprehensive client conceptualization that allows for appropriate medical referrals and psychological treatment planning.
Common screening tools
Migraine recognition tool: ID-Migraine Screener
- Structure: 3-item screening tool.
- Focus: Symptoms within the past 3 months, including nausea, sensitivity to light, and disability.
- Evidence: Demonstrates sensitivity, specificity, reliability, and validity. Its ease of use and operating characteristics suggest that it could significantly improve migraine recognition (Lipton et al., 2003).
Screening for functional impairment: Migraine Disability Assessment (MIDAS)
- Structure: 7 questions.
- Focus: Quantifies the extent to which migraine affects work or school, household chores, and social and leisure activities.
- Evidence: Brief, easy to use, valid instrument to assess headache-related disability, which makes it a useful tool in mental health screening (Steward, 1999).
Impact on daily life assessment: Headache Impact Test (HIT-6)
- Structure: 6 items.
- Focus: Designed to assess the impact of headaches on an individual’s daily life, including social, occupational, and psychological aspects.
- Evidence: Reliable and valid tool for discriminating the impact of headaches across episodic and chronic migraine (Yang et al., 2011).
Assessment of interictal burden: Migraine Interictal Burden Scale (MIBS-4)
- Structure: 4 items.
- Focus: The burden of migraine between attacks, including impairment in work or school, impairment in family and social life, difficulty making plans or commitments, and emotional/affective and cognitive distress.
- Evidence: The MIBS-4 has demonstrated good reliability and validity (Buse et al., 2009).
Disclaimers
Migraine screening tools are not diagnostic instruments by themselves. Instead, these instruments are resources that can be used (a) for the purposes of education or (b) to aid mental health professionals in their conceptualization, clinical treatment, and referral of clients.
Referrals to medical doctors or other qualified medical providers for full health screenings and diagnoses are critical. A thorough evaluation by a physician is needed to formally diagnose a migraine and prescribe a medical treatment plan.
The authors of this article make no claims or warranties about the completeness or effectiveness of the screening tools. This article only highlights a few of the several published screening tools currently available.
Treatment and intervention
Many people suffer for years without an accurate diagnosis or treatment for migraine. Effective interventions help validate the individual’s experience and offer empowerment through awareness and education. Further, therapy and support help them regain a sense of control over their health and their lives.
The biopsychosocial model
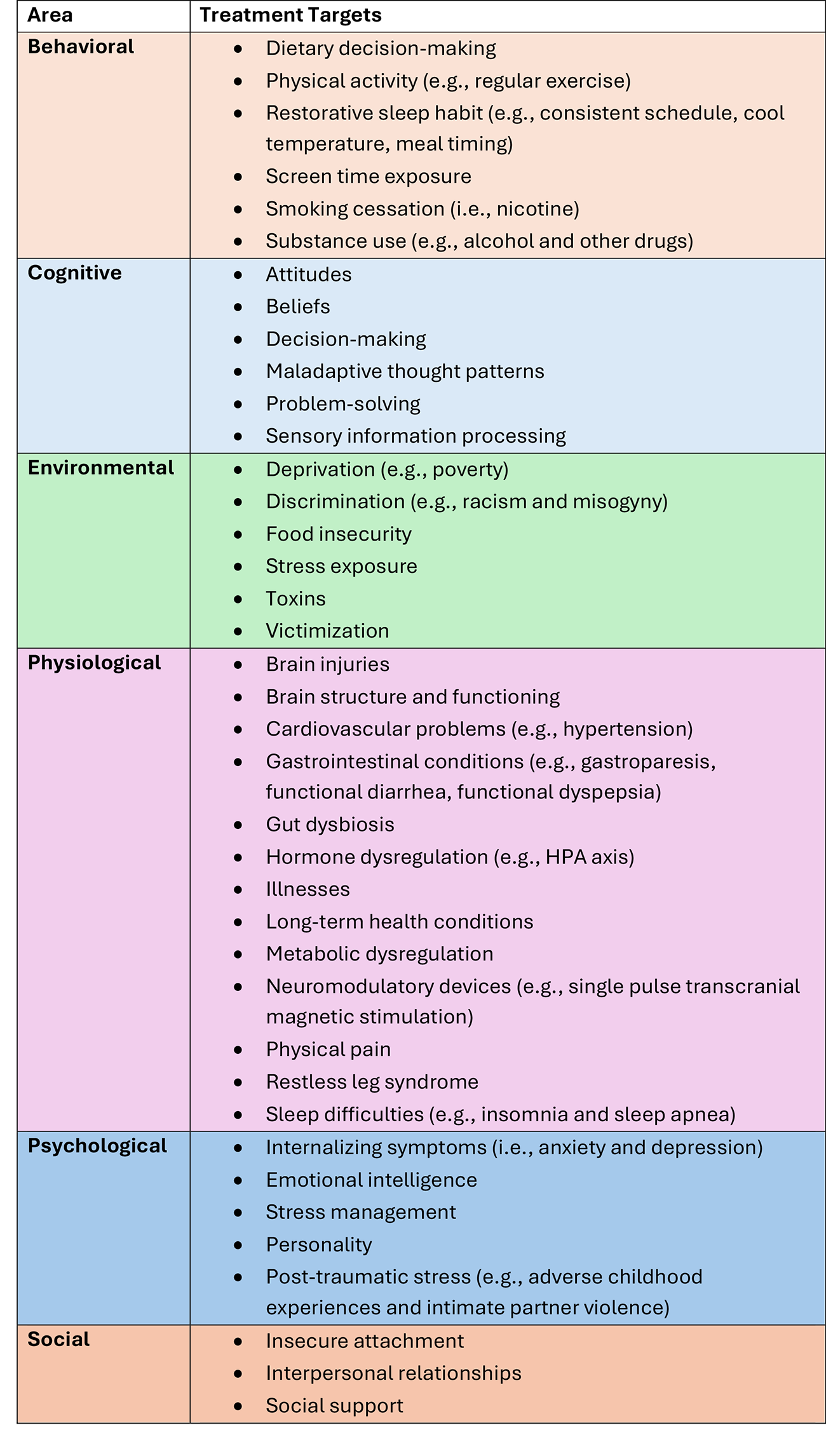
The biopsychosocial model is a holistic framework for understanding health and illness (Engel, 1977). This patient-centered perspective recognizes that physical and mental health conditions result from the interplay of biological, psychological, and social factors (Inan, 2024; for an overview, see Table 1). Given that migraine is a complex neurological condition influenced by many factors, adopting the biopsychosocial model may help improve the treatment and management of symptoms (Rosignoli et al., 2022). Specifically, careful consideration of a client’s individual symptoms, triggers, and needs can inform the development of a personalized treatment plan (Rosignoli et al., 2022). Persson and colleagues’ (2023) study highlights the wide variability in the character and location of migraine-related pain across patients. Table 2 provides an overview of behavioral, cognitive, environmental, physiological, psychological and social treatment targets that should be considered when using a biopsychosocial approach to migraine treatment (Aurora et al., 2021; Badaeva et al., 2023; Shabani & Ghari Saadati, 2019). The successful use of the biopsychosocial approach in treating chronic pain conditions through both conventional and non-pharmacological treatments could serve as a template for its application to migraine (Rosignoli et al., 2022).
Table 1. Biopsychosocial Model.
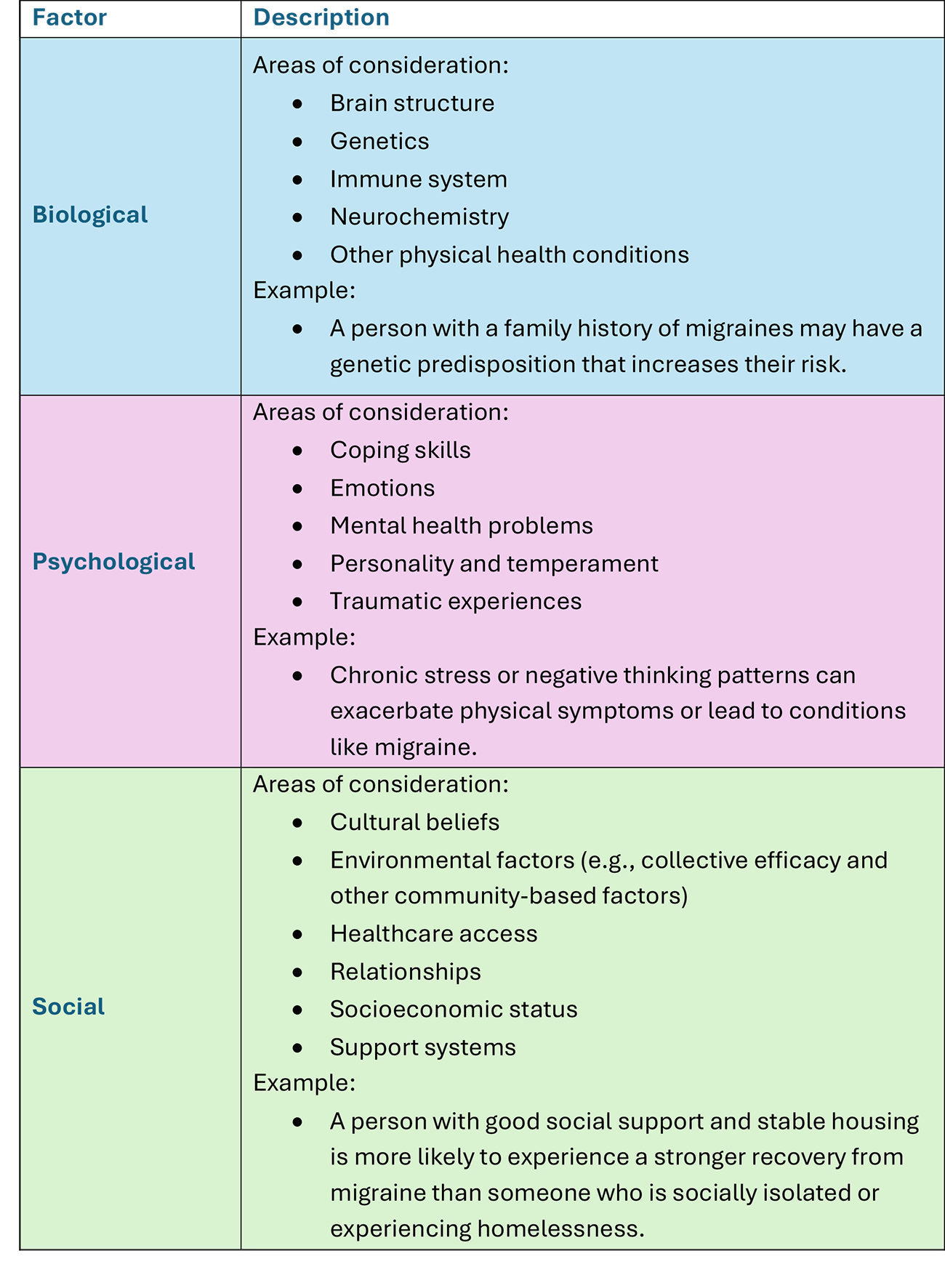
Table 2. Potential Biopsychosocial Approach-based Treatment Targets for Migraine.
Functional medicine insights
Functional medicine-based insights and approaches have the potential to help medical providers better understand and manage migraine symptoms (Institute of Functional Medicine, 2024). Mental health professionals can benefit from understanding functional medicine to make appropriate referrals for their clients. This framework is centered on identifying and addressing the root causes of ailments at an individual level. These can include genetic, environmental, and lifestyle factors. One such lifestyle factor is diet and nutrition, which has emerged as a key intervention target for clients with migraine (Badaeva et al., 2023; Cloyd, 2023).
A growing body of research has found that migraine symptoms are associated with the consumption of specific foods (Institute of Functional Medicine, 2024). Data show that food-related triggers are responsible for headache attacks in roughly 27–30% of migraine patients (Tu et al., 2025). As such, personalized nutritional interventions can help minimize or eliminate migraine symptoms. Qualified functional medicine clinicians can guide clients through an elimination diet to assess the effectiveness of this approach (Badaeva et al., 2023; Institute of Functional Medicine, 2024). Common food and beverage triggers include nuts, citrus, cheese, caffeine, chocolate, coffee, MSG, nitrates, tyramine, sulfites, aspartame, and alcohol (American Migraine Foundation, 2025; Gazerani et al., 2024; Hindiyeh et al., 2020; Tu et al., 2025). According to a systematic review, fasting can also act as a migraine trigger in 44% of migraine sufferers (Hindiyeh et al., 2020). Another promising dietary strategy to address migraine symptoms is the Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) diet, which has been linked to 36% reduction in the likelihood of headaches (Askarpour et al., 2020). Other treatment directions for medical providers include addressing hormone dysregulation (e.g., cortisol, melatonin, and estrogen), incorporating probiotics and supplements (e.g., vitamin D, magnesium, omega-3 fatty acids, and CoQ10), addressing histamine intolerance, and alleviating food insecurity (Badaeva et al., 2023; Cloyd, 2023; Izquierdo-Casas et al., 2019; Nagata et al., 2019). Future research grounded in functional medicine is needed to better understand the effectiveness of lifestyle-based interventions (e.g., neuronutrition) for managing migraines (Institute of Functional Medicine, 2024).


Strengthening interdisciplinary communication: The language of chronic health issues
The collaboration of interdisciplinary teams can play a crucial role in addressing migraine. This team-based approach can help improve how a client is holistically treated through a biopsychosocial lens. For instance, mental health professionals often lack training in chronic diseases, which leads to a gap in comprehensive client care. Similarly, many medical providers work in silos, limiting collaboration with mental health clinicians.
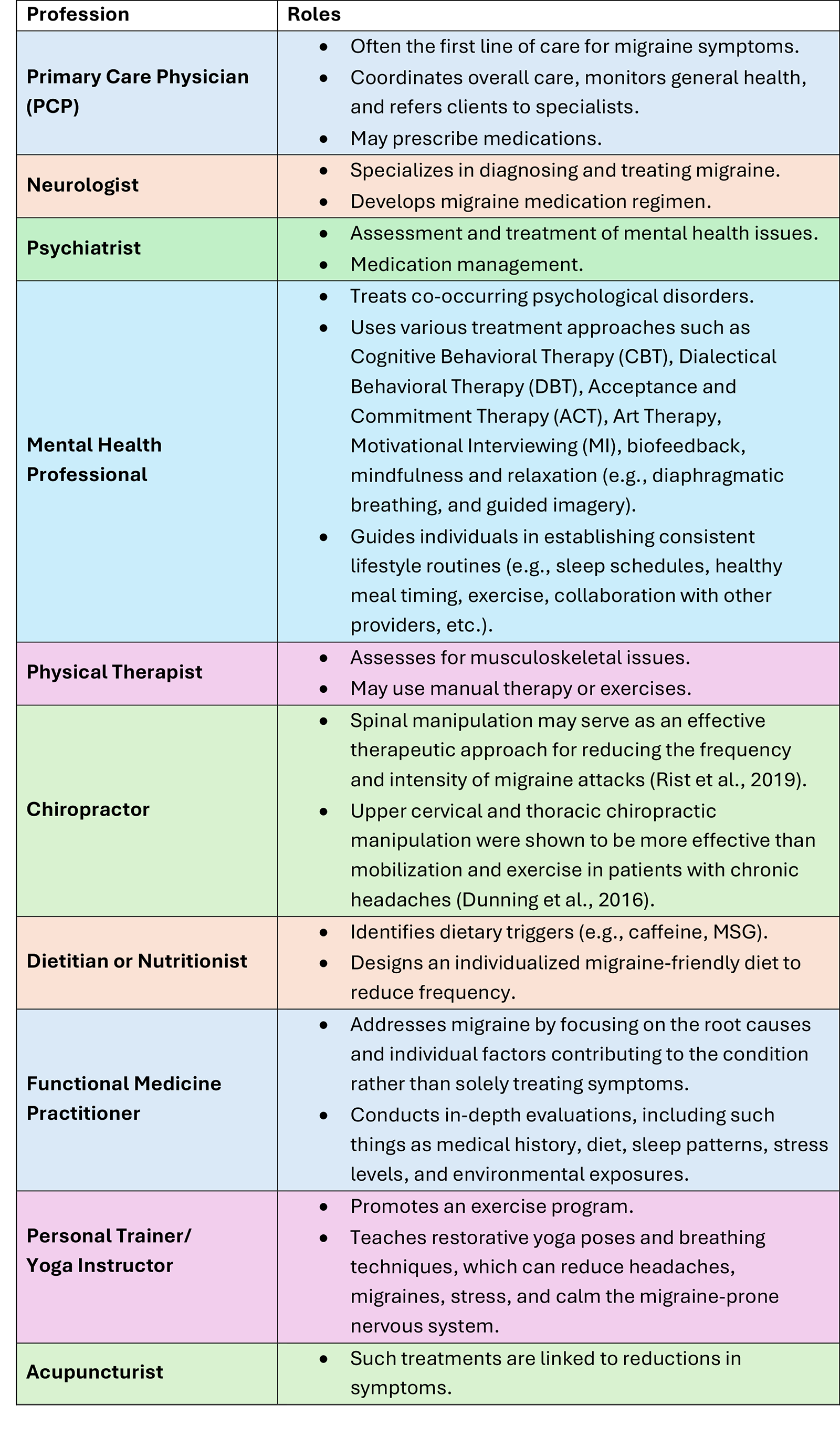
Mental health professionals can help improve communication to close this gap. A first step could be improving their basic understanding of medical terminology related to chronic conditions like migraine. This can empower clinicians to communicate more effectively with medical providers through discussions, assessments, and relevant case notes. In turn, mental health providers can also strengthen communication on topics including the impacts of lifestyle factors (e.g., sleep, diet, and stress) and mental health disorders on migraine, which many medical doctors overlook. Even as communication improves, it will remain critical for each professional to stay within their scope of practice and refer to allied professionals where appropriate (for an overview, see Table 3; Ling, 2024; Sturgeon et al., 2023).
Table 3. Examples of Allied Professionals’ Evidence-based Assessment and Treatment for Migraine.
Educational case study
Using the information outlined in this article as a lens, clinicians can better contextualize and inform treatment for the client. The fictitious clinical case study of Jane highlights the processes, challenges, and benefits of assessing and treating migraine through a biopsychosocial perspective.
Jane is a 55-year-old woman who was recently divorced. She presents with a history of recurrent migraine, which has occurred since she was an adolescent, and reports that her siblings also struggle with migraine. Her symptoms have increased in frequency and severity over the past few months. She reports migraine occurring one to two times per week. These episodes are often accompanied by nausea, which require her to retreat to a dark room. When symptoms escalate, she goes to the emergency room where treatment usually includes IV pain management fluids, cold compresses, and medications. Jane usually has difficulty with cognition, balance, appetite, dehydration, and light sensitivity in the day after a migraine. Experiencing measured, slow improvement, Jane typically “feels better” by day three. Even when recovered, Jane feels anxious about future migraine episodes.
Jane presents with the following comorbidities: environmental allergies, asthma, perimenopausal symptoms, anxiety, and sleep disturbances. She describes herself as a perfectionist who is continually critical of herself. Jane was raised in a family where seeking help for distress was stigmatized, and she briefly mentions having a difficult childhood with emotional and physical abuse. She is anxious about financial and emotional stressors lingering from her recent divorce. Jane reports high work-related stress, including long work hours, a poor diet, and inadequate sleep. She is concerned about her declining work performance, increasing irritability, and the impact her migraine experiences are having on her relationships and overall quality of life. Due to her long work hours, she lacks sufficient time for friendships.
Nutritional science considerations and key takeaways
Assessment and recommendations
When examining assessment considerations, mental health professionals are tasked with making referrals to qualified providers when the nature of a client’s needs fall outside their scope of practice. By working together with other qualified providers, the mental health professional can better understand the patient’s needs and create a treatment plan that supports their overall well-being.
It is vital that mental health clinicians are aware of the interventions a medical provider or licensed nutritionist may consider.
A few are presented below:
- Headache is the number one symptom of histamine intolerance; thus, a physician may assess for histamine intolerance (diamine oxidase (DAO) deficiency) (Izquierdo-Casas et al., ).
- Assess for the consumption of trigger foods, including nuts, citrus, cheese, caffeine, chocolate, coffee, MSG, nitrates, tyramine, sulfites, aspartame, and alcohol (American Migraine Foundation, 2025; Gazerani et al., 2024; Hindiyeh et al., 2020; Tu et al., 2025).
- Assess for cardiovascular risk factors, including hypertension, diabetes, high cholesterol, and obesity, as they are comorbidities of migraine (Hindiyeh et al., 2020).
- Assess for permeability of the gut (leaky gut; Arzani et al., 2020).
- Assess for deficiencies with magnesium, carnitine, riboflavin, niacin, CoQ10, vitamin D, Vitamin B12, and alpha lipoic acid (Nattagh-Eshtivani et al., 2018).
- A nutritionist may help a client eliminate specific foods, such as wheat, oranges, eggs, caffeine, cheese, chocolates, and milk (The IgG‐based elimination diet) (Hindiyeh et al., 2020).
- A different dietary interventions such as a low histamine diet, low glycemic diet, or the Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND), carbohydrate-restricted diets, ketogenic diets, vitamin D3 supplementation, omega-3 fatty acids, probiotic supplementation, and increased water intake (Institute of Functional Medicine, 2025; Arzani, 2020; Tu et al., 2025).
- Balance the Omega 3 to Omega 6 ratio to increase Omega 3 and reduce Omega 6 intake (American Migraine Foundation, 2025).
- Encourage 5-6 smaller meals throughout the day to prevent the feeling of hunger, which can trigger a migraine (American Migraine Foundation, 2025).
Behavioral health considerations and key takeaways
- Mental health providers are encouraged to improve their basic understanding of medical terminology, causal factors, and possible treatments related to chronic conditions like migraine.
- Knowledge empowers clinicians to communicate more effectively with medical providers through discussions, assessments, and relevant case notes.
- Mental health providers can also bolster their communication to clients on topics including the impacts of lifestyle factors (e.g., sleep, diet, and stress) and mental health disorders on migraine, which many medical professionals may overlook.
- Behavioral, cognitive, environmental, physiological, psychological and social treatment targets should be considered when using a collaborative biopsychosocial approach to migraine treatment (Aurora et al., 2021; Badaeva et al., 2023; Shabani & Ghari Saadati, 2019).
Conclusion: A step toward integrated care
Mental health providers have a responsibility to understand and recognize chronic health conditions like migraine and work collaboratively with other providers. Critical initial steps are (a) improving screening practices and (b) better understanding the language of migraine (e.g., key migraine classifications of severity and common symptoms). These steps will better equip clinicians to engage in meaningful discussions with other providers and more effectively advocate for their clients. Such a holistic approach to healthcare helps ensure clients receive comprehensive care that addresses both mental and physical health, and significantly improves client outcomes and quality of life.


Jerrod Brown, PhD, MA, MS, MS, MS, is a professor, trainer, researcher, and consultant with multiple years of experience teaching collegiate courses. Brown has completed four separate master’s degree programs and holds graduate certificates in Medical Biochemistry, Exercise Prescription, Neuroscience and the Law, Neuropsychology, Dyslexia, Autism Spectrum Disorder (ASD), Other Health Disabilities (OHD), and Traumatic-Brain Injuries (TBI). Currently, Brown is pursuing his fifth master’s degree in Applied Clinical Nutrition from Northeast College of Health Sciences.

Jeremiah Schimp, PhD, MA, LPCC, is an Assistant Professor of Psychology at Concordia University, St. Paul. He has taught psychology since 2016, specializing in counseling and psychopathology. He has worked in the mental health field since 2004, focusing his clinical career on adults diagnosed with serious and persistent mental illnesses and substance use disorders. Dr. Schimp holds a BA in Psychology, an MA in Counseling Psychology, and a PhD in Psychology with a specialization in health psychology. He is a Licensed Professional Clinical Counselor in the state of Minnesota and holds certifications in integrative mental health, addiction, and trauma.

Shelley Mydra, DMFT, LMFT, is an Adjunct Professor of Psychology at Pepperdine University Graduate School of Education and Psychology (GSEP). She holds a Doctorate and Licensure in Marriage and Family Therapy and has extensive clinical experience. In addition to being an AAMFT Board Approved Supervisor, she is certified in Lifestyle Medicine and Pain Neuroscience Education. She serves on the advisory boards of the GSEP Board of Visitors and the Impact Collaborative.

Leanne Skehan DCN, MSACN, MPH, MBA, holds a Doctor of Clinical Nutrition degree from Maryland University of Integrative Health. She is a full-time faculty member at Southern New Hampshire University in the Master of Public Health program and an adjunct instructor at Northeast College of Health Sciences in the Master of Applied Clinical Nutrition program. Dr. Skehan resides in Texas, where she operates a nutrition consultation business.

Bettye Sue Hennington, PhD, is a professor at the University of Mississippi Medical Center with 24 years of teaching experience in institutions of higher learning. Her research interest is in the field of metabolomics, specifically in the causes of low birth weight in newborns.

Stacey L. Mascia holds a Doctor of Literature and Criticism (Indiana University of Pennsylvania) and an MA in English (College of Saint Rose). She is Professor of English with a focus on Disability Studies at North Country Community College in Upstate, New York. She co-authored a memoir with her late sister, describing early childhood trauma, a contributor to their migraines.
Elija Kneringer, BS, is a therapy trainee currently pursuing a master’s degree in Clinical Mental Health Counseling, with an expected graduation in March 2026. Kneringer earned a bachelor’s degree in Human Physiology and holds a certificate in Exercise Physiology, as well as current CPR/AED certification. Kneringer’s clinical work focuses on supporting clients experiencing trauma, anxiety, migraines, and other neuropsychological impairments. With special interests in neuropsychology and forensic psychology, Kneringer is dedicated to integrating neuroscience-informed approaches into clinical practice, with particular attention to the mind-body connection in mental health.
American Migraine Foundation. (n.d.). Facts about migraine. Retrieved from https://americanmigrainefoundation.org/resource-library/migraine-facts/
American Migraine Foundation. (2025). Diet and headache control. https://americanmigrainefoundation.org/resource-library/diet/#:~:text=There%20is%20no%20one%20%E2%80%9Cright,prevent%20headaches%20due%20to%20hunger
Anderson, G. (2019). Integrating pathophysiology in migraine: Role of the gut microbiome and melatonin. Current Pharmaceutical Design, 25(33), 3550-3562.
Arzani, M., Jahromi, S.R., Ghorbani, Z. et al. (2020). Gut-brain Axis and migraine headache: a comprehensive review. J Headache Pain 21, 15. https://doi.org/10.1186/s10194-020-1078-9
Aurora, S. K., Shrewsbury, S. B., Ray, S., Hindiyeh, N., & Nguyen, L. (2021). A link between gastrointestinal disorders and migraine: Insights into the gut–brain connection. Headache: The Journal of Head and Face Pain, 61(4), 576-589.
Badaeva, A. V., Danilov, A. B., Clayton, P., Moskalev, A. A., Karasev, A. V., Tarasevich, A. F., … & Novikov, V. N. (2023). Perspectives on neuronutrition in prevention and treatment of neurological disorders. Nutrients, 15(11), 2505.
Balaban, H., Semiz, M., Şentürk, İ. A., Kavakçı, Ö., Cınar, Z., Dikici, A., & Topaktaş, S. (2012). Migraine prevalence, alexithymia, and post-traumatic stress disorder among medical students in Turkey. The Journal of Headache and Pain, 13(6), 459-467.
Buse, C., Rupnow, M., Lipton, R., (2009). Assessing and managing all aspects of migraine: Migraine attacks, migraine-related functional impairment, common comorbidities, and quality of life. Mayo Clin Proc, 84(5), 422-435.
Chen. J., Wang, Q., Wang, A., Lin, Z. (2020). Structural and functional characterization of the gut microbiota in elderly women with migraine. Frontiers in Cellular and Infection Microbiology, 9, 470.
Dimitrova, A. K., Ungaro, R. C., Lebwohl, B., Lewis, S. K., Tennyson, C. A., Green, M. W., Babyatsky, M. W., Green, P. H. (2013). Prevalence of migraine in patients with celiac disease and inflammatory bowel disease. Headache, 53, 344–355.
Dindo, L., Recober, A., Haddad, R., Calarge, C. (2017). Comorbidity of migraine, major depressive disorder, and generalized anxiety disorder in adolescents and young Adults. Int J Behav Med, 24(4) 528-534.
Friedman, D. I., & De Ver Dye, T. (2009). Migraine and the environment. Headache: The Journal of Head and Face Pain, 49(6), 941-952.
Gazerani, P., Papetti, L., Dalkara, T., Cook, C. L., Webster, C., & Bai, J. (2024). The brain, the eating plate, and the gut microbiome: Partners in migraine pathogenesis. Nutrients, 16(14), 2222.
Hindiyeh, N. A., Zhang, N., Farrar, M., Banerjee, P., Lombard, L., & Aurora, S. K. (2020). The role of diet and nutrition in migraine triggers and treatment: A systematic literature review. Headache, 60(7), 1300–1316.
Institute of Functional Medicine. (2025). Migraine, mast cells, & low-histamine diet. https://www.ifm.org/articles/migraine-mast-cells-low-histamine-diet
Izquierdo-Casas, J., Comas-Basté, O., Latorre-Moratalla, M. L., Lorente-Gascón, M., Duelo, A., Soler-Singla, L., & Vidal-Carou, M. C. (2019). Diamine oxidase (DAO) supplement reduces headache in episodic migraine patients with DAO deficiency: A randomized double-blind trial. Clinical Nutrition (Edinburgh, Scotland), 38(1), 152–158.
Karimi, L., Wijeratne, T., Crewther, S., Evans, A., Ebaid, D., Kahalil, H. (2021). The migraine-anxiety comorbidity among migraineurs: A systematic review. Frontiers in Neurology, 11.
Khan, J., Asoon, L. I. A., Sunni, A. A., Rafique, N., Latif, R., Saif, S. A., Almandil, N. B., Almohazey, D. & AdulAzeez, S. (2021). Genetics, pathophysiology, diagnosis, treatment, management, and prevention of migraine. Biomedicine & Pharmocotherapy, 139(2021), 1-15.
Ling, M. H. (2024). A 10-year systematic review (2013 to 2022) on effects of diet on migraine. EC Clinical and Medical Case Reports, 7, 01-15.
Lipton, R., Dodick, D., Sadovsky, R., Kolodner, K., Endicott, J., Hettiarachchi, J., Harrison, W. (2003). A self-administered screener for migraine in primary care: The ID migraine validation study. Neurology, 61(3):375-82.
Lipton, R., Buse, D., Friedman, B., Feder, L., Adams, A., Fanning, K., Reed, M., Schwedt, T. (2020). Characterizing opioid use in a US population with migraine: Results from the CaMEO study. Neurology, 4(95).
Marchiando, A. M., Graham, W. V. and Turner, J. R. (2010). Epithelial barriers in homeostasis and disease. Annual Reviews in Pathology, 5, 119–144.
Martami, F., Ghorbani, Z., Abolhasani, M., Togha, M., Meysamie, A., Sharifi, A., Jahromi, S. R. (2018). Comorbidity of gastrointestinal disorders, migraine, and tension-type headache: A cross-sectional study in Iran. Neurological Science, 39(1), 63-70.
Martami, F., Mansoureh, T., Seifishahpar, M., Ghorbani, Z., Ansari, H., Karimi, T., Jahromi, S. R. (2019). The effects of a multispecies probiotic supplement on inflammatory markers and episodic and chronic migraine characteristics: A randomized double-blind controlled trial. Cephalagia, 39(7), 841-853.
McCracken, H. T., Thaxter, L. Y., & Smitherman, T. A. (2024). Psychiatric comorbidities of migraine. Handbook of Clinical Neurology, 199, 505-516.
Mennigen, R. and Bruewer, M. (2009). Effect of probiotics on intestinal barrier function. Annals of the New York Academy of Science, 1165, 183–189.
Merrill, R., Gibbons, I. (2023) Comorbidity of sleep disorders, mental illness, and migraine or headaches. SN Compr. Clin. Med. 5(283).
Nagata, J. M., Weiser, S. D., Gooding, H. C., Garber, A. K., Bibbins-Domingo, K., & Palar, K. (2019). Association between food insecurity and migraine among US young adults. JAMA Neurology, 76(9), 1121-1122.
National Institute of Health. (2025). Migraine. National Institute of Neurological Disorders and Stroke. https://www.ninds.nih.gov/health-information/disorders/migraine#toc-phases-of-migraine-attack
Nattagh-Eshtivani, E., Sani, M. A., Dahri, M., Ghalichi, F., Ghavami, A., Arjang, P., & Tarighat-Esfanjani, A. (2018). The role of nutrients in the pathogenesis and treatment of migraine headaches: Review. Biomedicine & Pharmacotherapy = Biomedecine & Pharmacotherapie, 102, 317–325.
Rist, P. M., Hernandez, A., Bernstein, C., Kowalski, M., Osypiuk, K., Vining, R., Long, C. R., Goertz, C., Song, R., & Wayne, P. M. (2019). The impact of spinal manipulation on migraine pain and disability: A systematic review and meta-analysis. Headache, 59(4), 532–542.
Shabani, M., & Ghari Saadati, L. (2019). Comparison of the effectiveness of mindfulness-based cognitive therapy and quality of life therapy on perfectionism and rumination in patients with migraine. Avicenna Journal of Neuro Psycho Physiology, 6(1), 1-10.
Steward, W., Lipton, R., Kolodner, K., Liberman, J., Sawyer, J. (1999). Reliability of the migraine disability assessment score in a population-based sample of headache sufferers. Cephalalgia. 19(2), 107-114.
Sturgeon, J. A., Ehde, D. M., Darnall, B. D., Barad, M. J., Clauw, D. J., & Jensen, M. P. (2023). Psychological approaches for migraine management. Anesthesiology Clinics, 41(2), 341-355.
Tu Y-H, Chang C-M, Yang C-C, Tsai I-J, Chou Y-C, Yang C-P. (2025). Dietary patterns and migraine: Insights and impact. Nutrients, 17(4), 669.
van Hemert, S., Breedveld, A. C., Rovers, J. M., Vermeiden, J. P. W., Witteman, B. J. M., Smits, M. G., de Roos, N. M. (2014). Migraine associated with gastrointestinal disorders: Review of the literature and clinical implications. Frontiers in Neurology, 5, 241.
Walter, K. (2022). What is migraine? Journal of the American Medical Association. 327(1), 93.
Yang, M., Rendas-Baum, R., Varon, S., Kosinski, M. (2011). Validation of the Headache Impact Test (HIT-6) across episodic and chronic migraine. Cephalalgia, 31(3), 357-67.
Zhou, Y., Pang, M., Ma, Y., Lu, L., Zhang, J., Wang, P., Li, Q., Yang, F. (2024). Cellular and molecular roles of immune cells in the gut-brain axis in migraine. Molecular Neurobiology, 61(2), 1202-1220.
Other articles


The Silent Strain: Exploring the Emotional and Structural Burdens of Informal Caregiving
Unlike most roles in life, caregiving may be thrust upon individuals when they least expect it. In 2024, there were 105.6 million caregivers in the United States (Farmer & Ramchand, 2024), and in 2020, there were over 53 million unpaid caregivers supporting friends and loved ones with chronic conditions or disabilities (Centers for Disease Control and Prevention, 2024).
Srinithi Sridhar, MS & DeAnna Harris-McKoy, PhD

Resistance in Caregiving
Resistance is a common challenge in caregiving, experienced by both caregivers and care recipients. It often reflects a desire to maintain control and cling to the familiar, especially during times of stress or adversity. Care recipients may resist when they feel their independence is being taken away, while caregivers may feel overwhelmed and uncertain about how to respond. Family caregivers can also resist, especially when there is disagreement about care decisions, leading to conflict and tension.
Nancy L. Kriseman, MSW

Clinical Practice with Parents of Emerging Adults
Marlene, a 46-year-old mother, presents for therapy and tearfully tells you that her once solid relationship with her 19-year-old son is in jeopardy. Marlene proceeds to describe Erik’s pattern of “less than stellar grades,” “apathy about finding employment,” “staying out late,” and “using marijuana – a lot.” Marlene shares that her husband thinks “Erik is the way he is because I coddled him too much.”
Lynne Carroll, PhD & Paula J. Gilroy, EdD