
In the first half of 2022, AAMFT conducted an industry workforce study to examine the shifts related to COVID-19, their short- and longer-term impacts, and what challenges and opportunities are facing the field.
The Path to MFT
Historically, the path to marriage and family therapy has been varied. Influenced by the development curve of the profession, the timing of the evolution of licensure in the U.S., and the growth of training programs, in past years many entered marriage and family therapy as a second career. For some this was after they began careers in other mental health fields, but for many it was after working in unrelated industries.
In the 2022 study, while it remains true that many older respondents indicated they entered MFT as a second career, more early career professionals reported beginning their MFT studies immediately after undergraduate work.
Understanding potential shifts in how people are entering the field, as well as initially discovering marriage and family therapy, allows for stronger growth of the profession long-term‑—a particular focus because there are no undergraduate feeder programs dedicated to the study.
 Entry to the profession
Entry to the profession
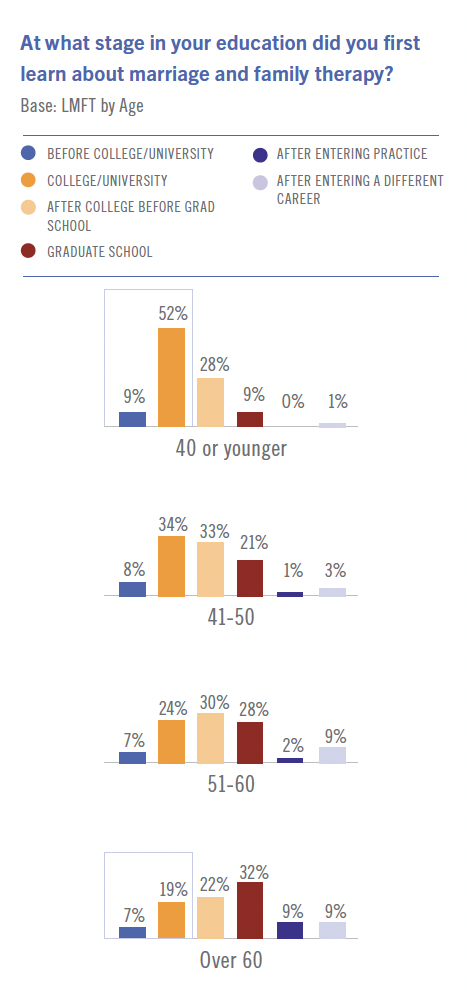
More than 2/3rds of licensed MFT respondents (68%) indicated they learned about marriage and family therapy after their undergraduate education. Segmentation revealed that LMFTs under 40 were more likely to learn about MFT before completing college/university (61%) compared to LMFTs over 60 (26%).
The top five professions of respondents who learned about marriage and family therapy after entering a different career path were counselor (20%), teaching/education (14%), ministry/pastoral (12%), arts/entertainment (12%), and business (12%).
About one-third of LMFTs were influenced to pursue marriage and family therapy by professors or teachers (33%) and classes/courses (30%). LMFTs working in a school/college/university setting were more likely than average to be influenced by professors or teachers (51%).
Because the marriage and family therapy field lacks a direct feeder program at the undergraduate level, and more people are starting training directly after receiving their bachelors’, targeting those in undergraduate programs with information about the profession will be vital to continue its growth.
>>Read part 1 here
>>To download the full report, visit aamft.org/workforcestudy
Attitudes about the profession
LMFT respondents commonly pursued the field because they agreed with the holistic approach of treating an individual in context with their personal relationship (56%) or they saw it as their calling or purpose (47%). Over a third (35%) also indicated they were drawn to the profession by a desire to make a positive social impact.
A strong majority (84%) of LMFTs reported they would be moderately or very likely to recommend marriage and family therapy as a career to a college student.
For those who indicated they would not recommend marriage and family therapy, the top reasons cited were low pay (41%), other disciplines/licenses more valued (37%), and limited scope and employment options (32%). Segmentation revealed that only 70% of agency LMFTs would recommend becoming an MFT as a career, compared to 94% of LMFTs in a school/college/university setting.
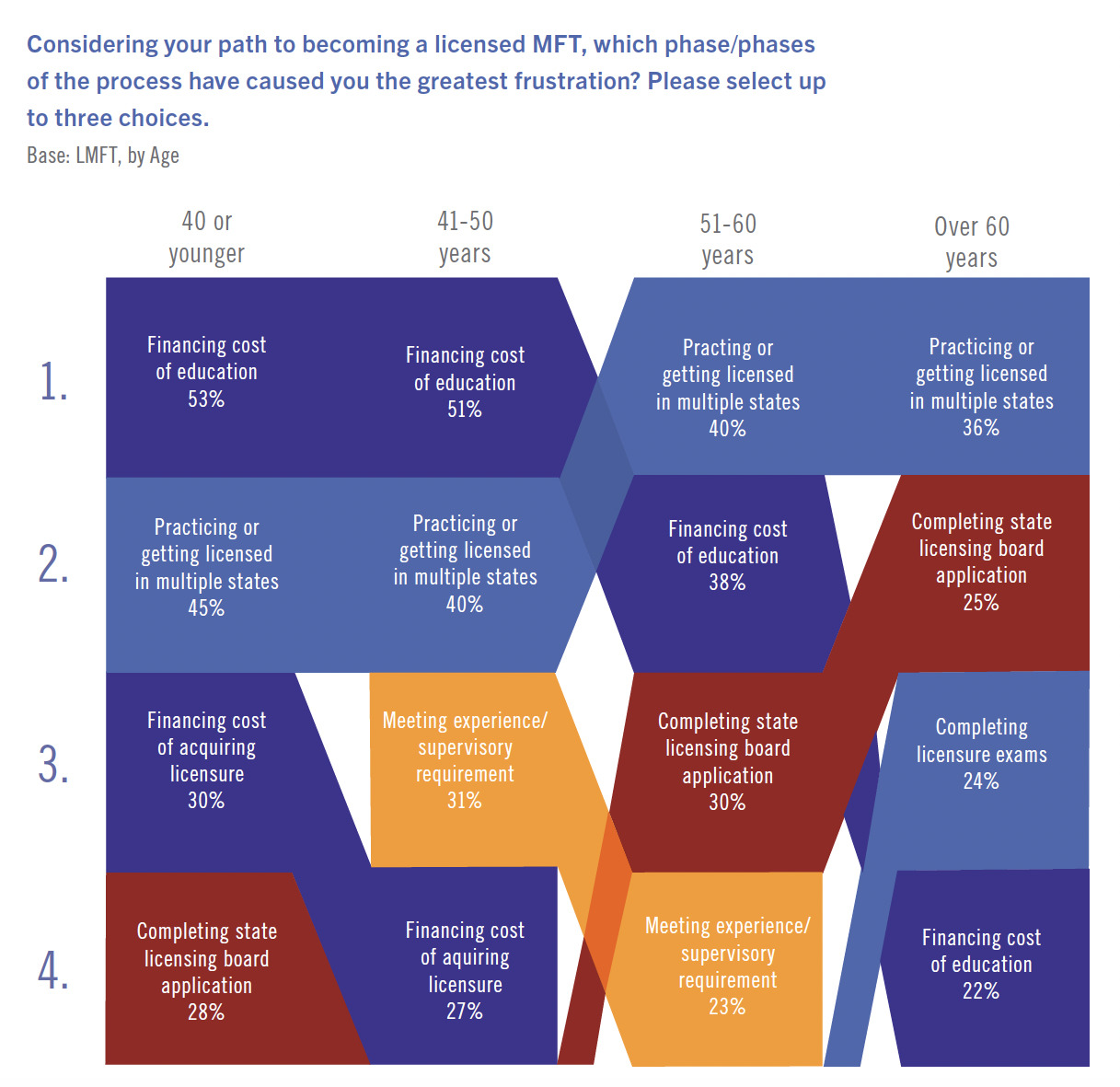
Frustrations in becoming an MFT
The greatest frustrations in the path to becoming a licensed MFT included financing the cost of education (39%) and practicing or getting licensed in multiple states (39%).
LMFTs were asked to identify what changes in the process would make it easier to become a licensed MFT; top responses included portability/reciprocity between states (35%), streamlined standard requirements (21%), financial assistance/less expense (16%), a better understanding of licensing process (12%), national licensing (12%), and more supervision/mentorship (11%).
Trends and Challenges for the Industry
It is evident that many of the changes the field has faced since the start of the COVID-19 pandemic are here to stay; telehealth and increased demands for mental health services chief among those. The paths forward from new and emergent challenges such as migrating clients and clinician burnout will need to be researched and assessed for how to find relief and solutions for the field.
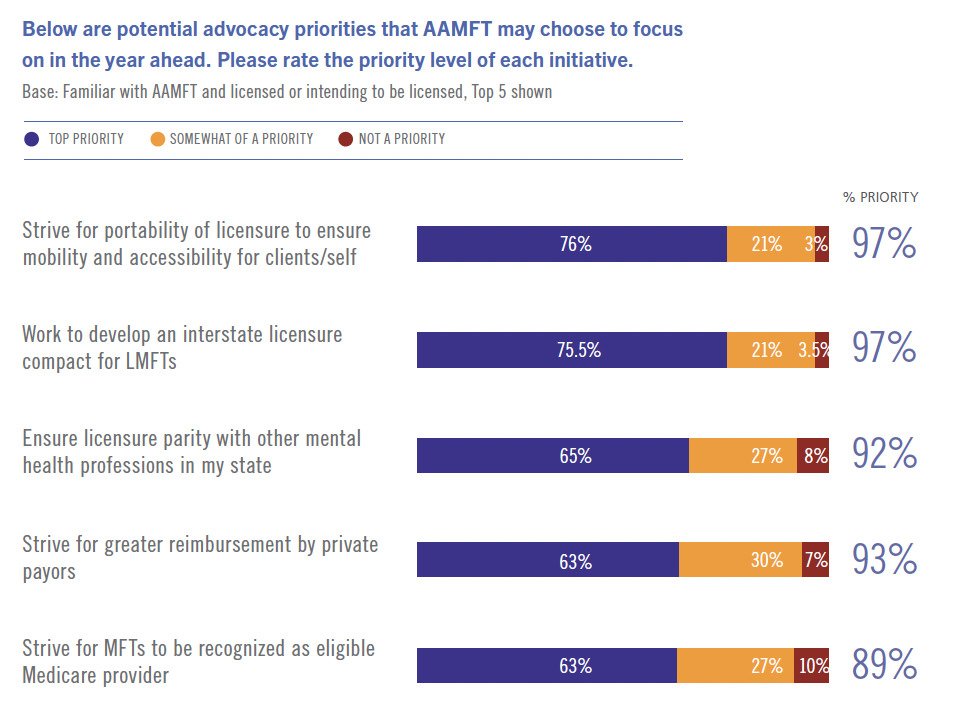
When asked to rate the importance of potential priorities for AAMFT to focus on in the year ahead, over three-fourths of respondents rated portability of licensure to ensure mobility and accessibility (76%) and development of an interstate licensure compact for LMFTs (76%) as top priorities. Nearly half (47%) of respondents identified strengthening advocacy efforts for greater employment opportunities for LMFTs as a top priority. These respondents were most interested in hospital (30%), school (27%), and government (19%) settings.
Employment

Almost two-thirds (63%) of LMFTs indicated demand for their services has grown as a result of COVID-19, with one third (34%) noting an increase in work hours because of the pandemic. About half (49%) reported working fully or partially remotely due to COVID-19.
Indications are that those currently in the field are at maximum capacity. Therapists reported spending an average of 21.8 hours a week delivering direct client services, just above the average of 20.4 hours they would like to spend delivering these services.
About half (46%) expected that the amount of time they spend delivering direct, clinical/therapeutic services will not change over the next year. Nearly one-third (32%) anticipated the amount of time spent on these services will increase, compared to just 17% of those who expect the amount of time to decrease.
A fifth (21%) of school/college/university LMFTs expected a significant increase in the time they spend delivering services over the next year.
With MFTs from every category reporting average clinical service hours above their desired amount, and most anticipating this situation will not change in the near term, potential burnout is a concern for the industry moving forward. In fact, over one-third (35%) of respondents indicated that burnout/managing a high client load was one of the top challenges facing the profession over the coming years.
Indications are that those currently in the field are at maximum capacity.
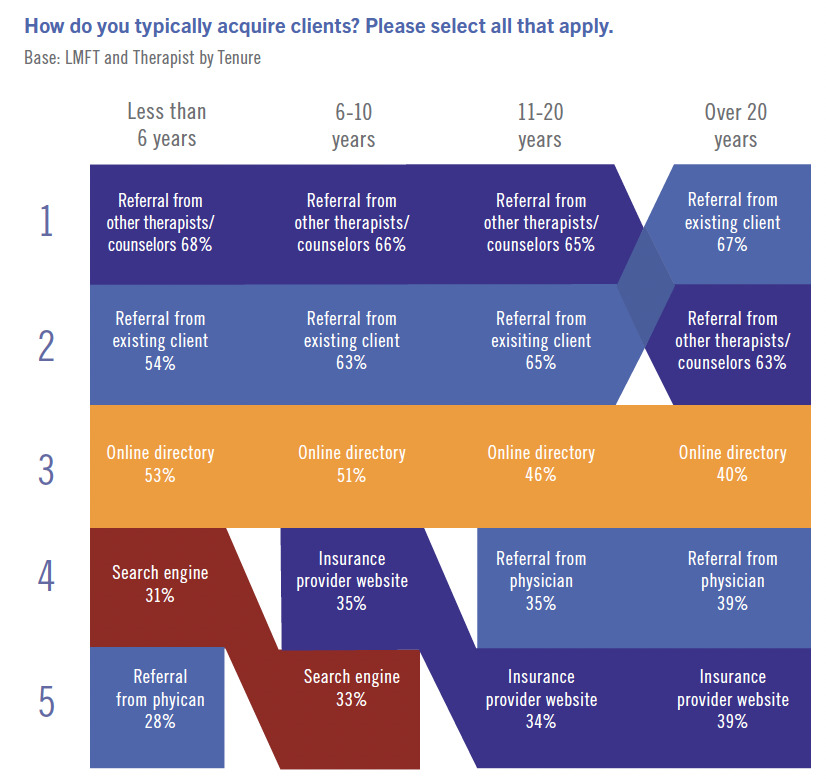
Client generation
While most respondents indicated they are at full employment, almost two-thirds of therapists responded, when necessary, they acquired clients from referrals from other mental health providers (64%) and existing clients (63%). Nearly half (46%) acquired clients from online directories. Segmentation revealed that therapists with less than six years of experience relied more heavily on online directories (53%) than those with over 20 years of tenure (40%), who were more likely to acquire clients from existing client referrals (67%) compared to those with less than six years of experience (54%).
Telehealth
The widespread use of telehealth is perhaps the largest shift in the profession coming out of the COVID-19 pandemic. Pre-pandemic, telehealth was practiced by a very limited number of therapists. Many considered telehealth as “second rate” or lacking substance.
A 2020 survey conducted by AAMFT indicated prepandemic, 58% of respondents were not using telehealth at all in their practices and only 4% were using it moderately or exclusively in their work.
In the 2022 workforce survey, nearly half (47%) of LMFTs reported seeing patients primarily (entirely or mostly) through telehealth. Over the next three years, a smaller percentage of LMFTs (39%) anticipate using telehealth as their primary format; however, nearly all (96%) plan to continue telehealth in some capacity.
This shift has some major implications for the industry. While most MFTs are now well-versed in its use, the rapid nature of the telehealth roll-out and the extensive use of now expired emergency orders as the guiding legal standards, indicate there is likely a need for all to develop a greater understanding of the laws, ethics, and best practices related to the method.

AAMFT is currently updating its telehealth best practice guidelines (anticipated publication date in 2023) as well as engaging in the preliminary stages of revising the AAMFT Code of Ethics.
There are also business implications for individual MFTs. Operating a hybrid practice of both in-person and telehealth clients while likely increasing access to care, requires the therapist to maintain business expenses related to both a physical office and a HIPAA-compliant telehealth platform. With younger professionals citing the financial burdens of low starting salaries and high student loan debt, it will be vital that cost effective ways are found to navigate this expanded business model.
Specializations
In their article “The Big Idea: The Age of Hyperspecialization” for the Harvard Business Review, Thomas W. Malone, Robert Laubacher, and Tammy Johns (2011) identified the labor market was entering into a new and not yet widely understood era of hyperspecialization.
The 2022 study reflected this era of labor evolution has in fact taken hold within the MFT field. Forty percent of respondents indicated they currently held a specialized credential with another 30% indicating they intended to pursue one. With those intending to pursue, the topic areas of greatest interest were Trauma/PTSD (53%) and Couples (43%).
Recognizing this emergent evolution, in 2017 AAMFT expanded its structure to offer mechanisms for hyperspecialization development via topical interest networks. Topics such as research, trauma, military, school and healthcare settings, and working with diverse client populations are currently included in the offerings, amongst other topics. All current offerings can be viewed at aamft.org/engage.
Reimbursement
Nearly half of all respondents (49%) identified getting fair private insurance reimbursement was a key challenge facing the profession.
Segmentation of responses revealed the following differences:
Membership: Former AAMFT members were more likely to rate private payor reimbursement as a top priority (69%) than current members (61%).
Job role: MFTs listing therapist as their primary role were also more likely to consider private payor reimbursement (65%) a top priority compared to students (56%) and academic researchers (47%). Students were also more likely to rate MFTs being recognized as eligible Medicare providers as a top priority (75%) compared to academic/researchers (69%) and therapists (59%).
Work setting: Agency LMFTs were more likely than those from other work settings to prioritize focus on striving for MFTs to be recognized as eligible Medicare and Medicaid providers (79%).
Recognizing this emergent evolution, in 2017 AAMFT expanded its structure to offer mechanisms for hyperspecialization development via topical interest networks.
Multi-state licensure
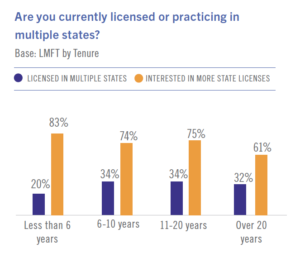 A growing need to service clients over state lines was another top challenge identified by 48% of respondents. Similarly, a vast majority of respondents (71%) indicated interest in multi-state licensure. Within the respondents, 31% indicated they currently practice in more than one state.
A growing need to service clients over state lines was another top challenge identified by 48% of respondents. Similarly, a vast majority of respondents (71%) indicated interest in multi-state licensure. Within the respondents, 31% indicated they currently practice in more than one state.
83% of LMFTs with less than 6 years of experience were interested in being licensed in more states, compared to just 61% of respondents with over 20 years of tenure. Those with less than 6 years of experience were also less likely to already hold a second license (22%) compared to their counterparts (32-34%).
Less tenured LMFTs are likely still building their career and client portfolio and may thus be more interested in practicing in additional states as well. More tenured LMFTs have had time to pursue additional state licenses, and thus may be more satisfied with the number of licenses currently held.
Respondents most commonly indicated they currently held a second license in California (11%), Florida (8%), Washington (5%), and New York (5%).
Florida (22%), California (21%), and New York (18%) were also the top three cited states where respondents were interested in obtaining a second license.
With few exceptions, interest in multi-state licensure generally appears to be for bordering states.
When asked about a preference in method for easing the process of obtaining licensure in other states, respondents showed a preference for greater portability (44%) over the development of an interstate licensure compact (38%).
These data points are rather interesting when viewed alongside the responses that most LMFTs indicated they were at full-employment and were averaging more clinical client hours than they desired. Through interviews and focus groups as part of this and another project, the driving factor for having multiple state licenses was not financial. Rather, clinicians cited that they wanted to maintain current client relationships (continuity of care). While such reasoning makes sense given the current post-pandemic context, it does beg the question, “Will therapists maintain this perspective as they reduce their client hours to a more manageable state?” Further, if financial reasons are not the driving force, then will therapists want to keep paying for a second license, learning separate state regulations, and all the nuances that accompany practice across state lines?
Conclusion
While many of the trends identified in this study are indicative of those facing other industries, there are some unique aspects facing the profession in the coming years. Maximizing resources to address these challenges will be instrumental to the strength and growth of the MFT profession.
A key takeaway from the study was a desire for increased advocacy efforts related to licensure portability, parity with other mental health disciplines, and reimbursement. AAMFT’s Practice Protection Fund (PPF) is designed to help support vital growth efforts like these, as well as work against threats and challenges to the profession. Unfortunately, it is supported by less than a quarter of licensed MFTs in the U.S. Please donate to this vital work by texting PPF to 53-555 or visiting givebutter.com/PPF!
Other articles

Perspectives
Systemic Supervision
Systemic thinking is understanding and exploring the intricacies of an individual and bearing in mind how we impact each other through our interactions and behaviors. Applying this to therapy and supervision can be seen through acknowledging differences in belief systems, attitudes, and approaches to life.
Eman Tadros, PhD and Anjelica M. Nelson, MAEd

Perspectives
Myths About Marriage
There are many common misconceptions about what happens in marriage—myths that never come true—and behaviors flow from those myths that harm the couple and their relationship, leaving them unhappy and dissatisfied. Statistics suggest that “happily ever after” occurs no more than 50% of the time, considering how many couples’ divorce.
Alan J. Hovestadt, EdD and Kenneth W. Schmidt, JCD

Perspectives
Integrating EMDR and EFT in Couple Therapy
As much as I’ve loved Eye Movement Desensitization and Reprocessing (EMDR) therapy and revolved my clinical practice around it, it has always felt like it has had one major short-coming; it has primarily been practiced as an individual therapy.
Jason N. Linder, PsyD