
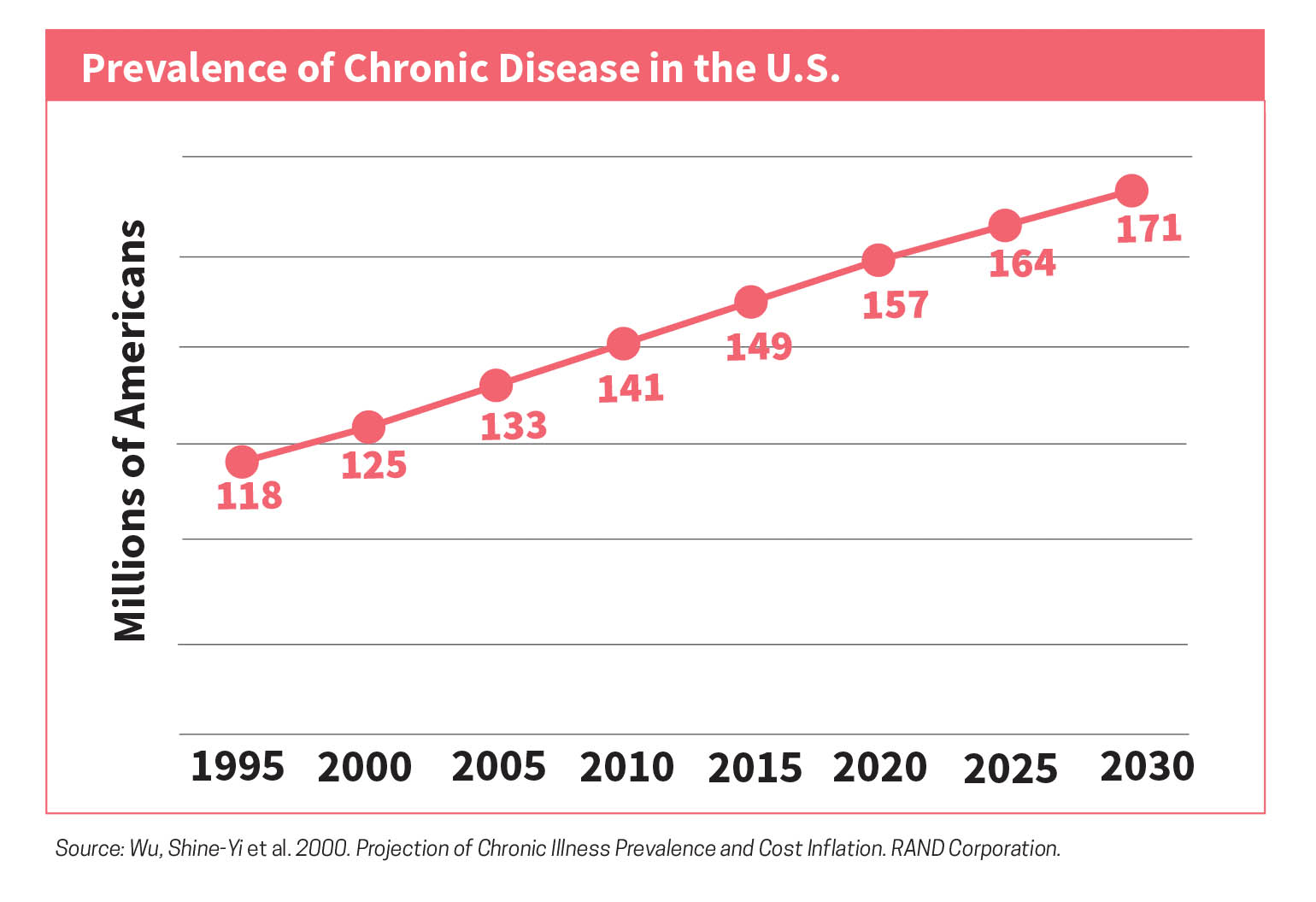
The Centers for Disease Control and Prevention (CDC, 2018) in a recent survey found that approximately 54.4 million people in the United States had been diagnosed with an arthritis related disease by a physician. Doctors focus on the individual patient when managing a chronic illness, but a diagnosis of a chronic illness reaches further than the individual alone.
Additionally, women are at a greater risk for developing an arthritis related illness. The illness can change the individual’s relationship with their family and friends and shift roles of loved ones to aid in the treatment of the chronic illness. This can cause additional complications for mothers caring for young children.
Diagnosis and assessment
When initially working with an individual and their family through therapy, it is imperative to gain an understanding of the illness, its management, history, prognosis, and what it means to the individual and the family. In their experimentation, Ireland and Pakenham (2010) found that a good predictor of the child’s adjustment depended on the illness onset; gradual onset correlated with more difficulties, poorer health, and lower social behaviors. For a therapist, it would be beneficial to understand how the individual, spouse, children, and external family adjusted or are continuing to adjust to the illness. It is also important to gain knowledge of any prior experience with chronic illness within the family, as that can alter perceptions of the individuals involved in treatment. Additionally, the individual perception each family member has regarding the impact of the illness can also shape the way the illness is addressed, as well as the amount of support the individual receives.
Another important factor to consider when working with the individual and family is the timeframe of the illness and diagnosis. Many individuals suffer for years before they obtain a proper diagnosis and then another year or two adjusting to the diagnosis and management of the disease. Chen and Fish (2013) indicated that a newer diagnosis typically correlated with more impairment and the individual spending more time managing their illness, and required more assistance in daily functioning. Having this understanding can help a therapist be more aware of the client’s capacity for treatment. What many therapists typically considered resistance during treatment is often clients feeling overwhelmed due to the illness and a diminished capacity to take on anything else, including attending a therapy session. The illness severity is also a significant factor in working with an individual and family. There are many types of illness and not all are difficult to consistently manage. Many diseases do not remain consistent and can include flares where the individual can be well managed and have a sudden flare-up which causes them to be at their worst in regard to the illness.
Understanding the frequency of good days versus bad days and what the client’s triggers are can help with the management of not only the illness, but throughout the therapeutic process. In addition, it is important to have knowledge about treatment requirements and medical procedures that a patient must endure to manage the illness itself or address complications due to the illness. These factors can be a struggle to share with the individual’s partner or spouse and even harder to share with any children in the home. Utilization of the biopsychosocial model at the start of treatment to obtain the necessary information regarding the client’s illness, coping, and support system is a necessity. Many therapists utilize the biopsychosocial model when working with clients. However, utilizing this model when working with the chronically ill population requires the therapist to delve deeper into the history to gain a better understanding of the clients daily functioning with their illness, and any impairments, as well as their experience with the chronic illness.
Treatment options and biomedical issues
There have been several studies on specific therapeutic models used when working with chronically ill patients and their families, all of which note the importance of including the family in the treatment as the illness has a major role on the family unit.
Hodgson, McCammon, Marlowe, and Anderson (2012) discussed the importance of incorporating the spouse and family in addition to individual therapy: “this is often the greatest need in medical settings where behavioral health services are already in place but no one specializes in working with couples and families therapeutically” (p. 8). The Illness/Non-Illness Treatment Model is based on therapy broken down into four components: Building Rapport, Differentiation/Integration Work, Differentiation Work with attitudes, and Illness/Non-Illness themes (Navon, 2005). The main theme of this therapeutic model is to help the client differentiate between what is the illness language, such as physical symptoms and illness management, to non-illness language of thoughts and feelings. The therapist’s goal is to help the client shift the focus from what cannot be changed to what can be changed.
The utilization of solution-focused therapy is prominent as the therapist looks for exceptions in a client’s all or nothing thinking. This model is meant to open the dialogue of illness and then leads the way for therapists to implement various therapeutic techniques. Emotionally focused therapy (EFT) has shown to have benefits in building on the attachment of the spouse and family when an individual is experiencing a chronic illness. The implementation of EFT among chronic illness patients and their partners increases communication and attachment styles between them, which in turn helps the management of the illness itself (Kowal, Johnson, & Lee, 2003).
Medical family therapy (MedFT) has shown to be extremely successful when working with chronic illness, specifically cancer patients in hospital settings. Individuals who were previously reluctant to see the benefits of medical family therapy noted that “MedFT offered a calm and consistent presence, especially when medical providers were perceived as being too busy to attend to patient’s and family members emotional and psychological needs” (Hodgson, Lamson, Mendenhall, & Crane, 2012). Another approach is utilizing FSI model (Family Systems Illness Model) that focuses on the family system when a member is living with a chronic illness (Rolland, 2018). With all the models, it is important to gain an understanding of the medical status, treatments, and medical history at the start of therapy to obtain a better sense of where the client and the family are.
It is imperative for the mental health professional to have a good understanding of chronic illness and the impact illness can take on the individual and family. It is equally imperative that medical professionals treating the illness have a better understanding of quality of life, mental health status, and mental health management. The focus needs to shift and allow medical professionals to see the importance of collaborating with mental health professionals to provide patients with the best care possible (Linville, Hertlein, & Lyness, 2007). For most people diagnosed with a chronic illness, mental health is rarely addressed among the medical professionals working with the patients. Furthermore, for many medical professionals, managing the illness must fit within their scope of management and rarely do they take into consideration the patient’s own quality of life. Several of the participants in Robinson’s study described adjusting the management of their illness to fit within their life, versus the typical medical approach of making life fit the treatment (2017). This shift in thinking about the illness and the approach to management can aid in how the individual and family perceive the illness and can create better communication and expectations.
It is imperative that mental health professionals, as well as medical professionals, shift from the individual to the family when it comes to chronic illness. The research has shown that the family is equally impacted by the chronic illness, yet the healthcare system focuses the treatment and support on the individual with the illness (Berry, Davies, & Dempster, 2016). In addition, many of the services provided for chronically ill patients focus on the short-term immediate management of the illness or diagnosis which leads to the long-term needs of that individual and family being overlooked (Chen & Fish, 2013). Helping the individual and the family look ahead and anticipate obstacles that might arise because of the illness is essential in its management.
 One of the most important factors in achieving this is to help the individual and family maintain a positive attitude and outlook on their illness and abilities, regardless of the negative impact the illness may have. Research has shown that having gratitude and forgiveness increased the psychological and physical quality of life, as well as improved overall life satisfaction in an individual’s suffering from a chronic illness (Eaton, Bradley, & Morrissey, 2014). In addition to improvements in the quality of life, having a positive outlook and gratitude can improve interactions with the spouse, family, and children of the chronically ill individual.
One of the most important factors in achieving this is to help the individual and family maintain a positive attitude and outlook on their illness and abilities, regardless of the negative impact the illness may have. Research has shown that having gratitude and forgiveness increased the psychological and physical quality of life, as well as improved overall life satisfaction in an individual’s suffering from a chronic illness (Eaton, Bradley, & Morrissey, 2014). In addition to improvements in the quality of life, having a positive outlook and gratitude can improve interactions with the spouse, family, and children of the chronically ill individual.
All too often, people suffering from a chronic illness focus on the things they can no longer do and feel helpless which leads to depression. Individuals suffering from a chronic illness struggle with limitations of caring for their children and participating in activities with them. Chen and Fish (2013) discuss that “while parents living with chronic illness may not able to attend school meetings or help children with homework, their attitudes toward their children’s academic achievement (e.g., academic aspiration and expectations) may play a particularly important role in their children’s academic functioning” (p. 15). This can lead to a lack of engagement with their children which puts the child at risk academically, as well as psychologically and physically. This is where the mental health professional can assist clients in changing their thought process around the illness and its limitations. Helping the individual find ways to work around the impact of illness can be challenging. This is where a good understanding of the impact of the illness, as well as the individual’s experience and perception of the illness, along with the family’s input, is crucial when working with an individual living with a chronic illness. By finding solutions to the limitations with the individual and family, they can feel more empowered and in control over their lives and illness. This positive outcome can then improve the overall quality of life and allow the individual and family to feel stronger and more united against future obstacles.
This article is offered free by AAMFT. If you are interested in accessing other content, join today!
Understanding the frequency of good days versus bad days and what the client’s triggers are can help with the management of not only the illness, but throughout the therapeutic process.

Julie Payne, MA, is a licensed marriage and family therapist in California and Texas. Payne is a Clinical Fellow of AAMFT. She has been working with clients suffering from chronic illness and trauma for over 15 years. She has spoken at several conferences for the Arthritis Foundation regarding mental health and chronic illness. In addition, she has held positions on the board of Houston Association for Marriage and Family Therapists as secretary and Long Beach South Bay chapter of California Association of Marriage and Family Therapists as secretary and 2018 president.
REFERENCES
Berry, E., Davies, M., & Dempster, M. (2017). Exploring the effectiveness of couples interventions for adults living with a chronic physical illness: A systematic review. Patient Education and Counseling, 100(7), 1287-1303.
Centers for Disease Control and Prevention. (2018). National statistics. Retrieved from https://www.cdc.gov/arthritis/data_statistics/national-statistics.html
Chen, Y., & Fish, M. (2013). Demands of maternal chronic illness and children’s educational functioning: An exploratory study. Child & Adolescent Social Work Journal, 30(3), 257-274.
Eaton, R., Bradley, G., & Morrissey, S. (2014). Positive predispositions, quality of life and chronic illness. Psychology, Health & Medicine, 19(4), 473-489.
Hodgson, J. L., McCammon, S. L., Marlowe, D. P., and Anderson, R. J. (2012). Medical family therapy in cancer care: Patient and family experiences. American Journal Of Family Therapy, 40(3), 258-266.
Hodgson, J., Lamson, A., Mendenhall, T., & Crane, R. (2014). Medical family therapy: Advanced applications. Springer.
Ireland, M. J., and Pakenham, K. I. (2010). Youth adjustment to parental illness or disability: The role of illness characteristics, caregiving, and attachment. Psychology, Health & Medicine, 15(6), 632-645.
Kowal, J., Johnson, S. M., & Lee, A. (2003). Chronic illness in couples: A case for emotionally focused therapy. Journal Of Marital And Family Therapy, 29(3), 299-310.
Linville, D., Hertlein, K., & Lyness, A. (2007). Medical family therapy: reflecting on the necessity of collaborative healthcare research. Families, Systems & Health: The Journal Of Collaborative Family Healthcare, 25(1), 85-97.
Navon, S. (2005). The Illness/Non-Illness treatment model: Psychotherapy for physically ill patients and their families. American Journal Of Family Therapy, 33(2), 103-116.
Robinson, C. A. (2017). Families living well with chronic illness: The healing process of moving on. Qualitative Health Research, 27(4), 447-461.
Rolland, J. (2018). Helping couples and families navigate illness and disability: An integrated approach. The Guliford Press.
RESOURCES
Hodgson, J., Lamson, A., Mendenhall, T., & Crane, R. (2014). Medical family therapy: Advanced applications. Springer. This book is an updated version of the book published in 1992. It focuses on advanced applications and updated content of working within MedFT. It is a resource for any clinician working with families experiencing a chronic illness.
McDaniel, S. H., Hepworth, J. & Doherty, W. J. (1997). The shared experience of illness. New York, NY: Basic Books. This book contains clinical cases of therapists working with chronically ill clients and how their own relationship with chronic illness shapes the work they do with their clients. The book illustrates a medical family therapy approach with a wide range of illnesses. This book also addresses the growing need for collaborative care amongst mental health clinicians and medical professionals.
McDaniel, S. H., Hepworth, J., & Doherty,W. J. (1992). Medical family therapy: A biopsychosocial approach to families with health problems. New York, NY: Basic Books. This book depicts the medical family therapy model and utilization of the biopsychosocial approach in working with chronic illness. The book discusses case examples and illustrates the importance of collaborative care with medical professionals and mental health providers. It also discusses the importance of the family systems approach and the role the family plays with an ill patient.
Rolland, J. (2018). Helping couples and families navigate illness and disability: An integrated approach. The Guliford Press. This book discusses the importance of working with families where one member has a chronic illness. It is an excellent resource for providers to help enhance their understanding of working with families experiencing a chronic illness.
Wright, N. H., & Ellis, L. (2010). Coping with chronic illness. Eugene, OR: Harvest House. This book is written by a therapist and researcher with first hand experience of living with a chronic illness. It provides ways to manage relationships with other family members as well as their treating physicians. It also provides useful coping techniques that have been helpful in managing symptoms relating to stress and depression due to the chronic illness.
Other articles

Perspectives
Equity and e-Learning for Children: Therapists as Advocates
Marcus, a 49-year-old widower and a single parent, was referred to therapy because he was concerned that his 10-year-old son, Edwin, and 13-year-old daughter, Bita, lagged behind academically during Spring 2020 distance learning. Marcus works two jobs and cannot be available to help his children stay on task with schoolwork due to his work schedule.
Bahareh Sahebi, PsyD and Mudita Rastogi, PhD

Perspectives
Integrative Approaches to Play Therapy
Symptoms of ADHD may be diminished using the Gottman Method when integrated with Reality Play Therapy (RePT) and/or Circus Arts Therapy fitness and play therapy program (CAT). While participating in play therapy, the therapist may utilize questioning methods from the Gottman Sound Relationship House’s (SRH; Gottman & Silver, 2015) seven phases in supporting parents and children to discover more about one another.
Sandra Fragomeni, MA and Michael Whitehead, PhD

Perspectives
Teaching Clients How to Argue Properly with the Use of Reflective Listening: A Worksheet
Picture this … a couple in your office is arguing. One starts to dominate the session with a filibuster onslaught, berating the other partner, because you waited a hair too long to interject while observing their negative interaction pattern. Now you’re scrambling to take back control of the room. . Sound familiar?
Lauren Kymberly Hill, MS