
Shelly tried everything. Melatonin. White noise. Blackout curtains. A sleep tracker that glared at her from the nightstand like a Cheshire cat. By the time she started seeing me, she had not slept more than four hours a night for three years; and her marriage was quietly unraveling. Her husband, Jared, had decamped to the guest room without discussion. They just stopped sleeping together, and somewhere in that silence, they stopped reaching for each other in other ways too.
In a previous article for Family Therapy Magazine (April 2026), I argued that MFTs are uniquely positioned to treat sleep disorders and that the relational context of sleep is not peripheral to the clinical problem but central to it. This article takes that argument further. Sleep anxiety generates a predictable set of relational dynamics. MFTs are well-equipped to address them. They just need a clinical map.
Sleep anxiety is not just insomnia
When couples present with sleep difficulties, we default to insomnia as the organizing diagnosis. But sleep anxiety is a meaningfully different entity and treating it as ordinary insomnia is one of the primary reasons clients plateau.
Insomnia is fundamentally a disorder of sleep. Sleep anxiety is fundamentally a disorder of fear: the nervous system has learned to treat the bedroom, the act of lying down, and the approach of bedtime as signals of threat. A significant proportion of treatment-resistant insomnia is driven by this threat-perception mechanism, and fear requires its own treatment logic (Forman, 2026).
The difference is clinically consequential. For the insomnia sufferer, the bedroom is frustrating. For the sleep-anxious client, it is construed as dangerous. One lies awake wishing for sleep; the other lies awake dreading it.
Three domains, three clinical pictures
In my theoretical work on sleep anxiety, currently in preparation, I identify three distinct domains. Understanding which is active is the foundation of accurate assessment.
 Fear of sleeplessness is the most common presentation, and the one most likely to show up in an MFT’s office masquerading as a “communication problem” or an “intimacy issue.” These clients dread lying awake. They run catastrophic predictions about tomorrow before they turn off the light, monitoring their bodies for signs of sleepiness the way an anxious client monitors a worrisome symptom. Sleep has become a performance and they believe they are failing.
Fear of sleeplessness is the most common presentation, and the one most likely to show up in an MFT’s office masquerading as a “communication problem” or an “intimacy issue.” These clients dread lying awake. They run catastrophic predictions about tomorrow before they turn off the light, monitoring their bodies for signs of sleepiness the way an anxious client monitors a worrisome symptom. Sleep has become a performance and they believe they are failing.
Fear of sleep itself is less common but more severe, and almost always missed because clinicians don’t ask the right questions. These clients aren’t afraid of lying awake. They are afraid of falling asleep: losing consciousness, losing voluntary control, crossing the hypnagogic threshold where the mind begins to let go. A history of abuse, sleep paralysis, hypnagogic hallucinations, or distressing nightmares can produce this presentation, as can a broader fear of vulnerability. These clients often manage by staying in lighter sleep—partial vigilance as a compromise between rest and safety.
Dysregulation of the nighttime nervous system is the domain most directly relevant to body-based and attachment-informed MFT work. The problem is autonomic: the nervous system cannot access the parasympathetic state that sleep onset requires. The sensations of physiological downregulation: slowing breath, relaxing muscles, and fading awareness have become threat cues rather than transition signals. A clinically important subgroup experiences relaxation-induced anxiety (RIA): the very act of trying to relax activates their nervous system rather than soothing it (Hazlett-Stevens & Craske, 2003). If you have ever prescribed a deep-breathing exercise that made a client more anxious, you have met this profile. Standard relaxation interventions are contraindicated without prior preparatory work.
The relational architecture of sleep anxiety
Sleep anxiety does not only live inside a single person. It lives in routines, silences, and accumulating accommodations. The relational system organizes around the anxiety in ways that are caring in intent and maintaining in effect.
The couple system is not the context in which sleep anxiety occurs. It is part of the mechanism.
Relationship quality is among the most powerful predictors of adult sleep quality, operating through both psychological and physiological pathways (Troxel et al., 2007). My systematic review of couple- and family-based sleep interventions found that partner involvement consistently moderated treatment outcomes, with attachment security and perceived partner responsiveness among the strongest predictors of change (Forman, in press). The couple system is not the context in which sleep anxiety occurs. It is part of the mechanism.
Three relational dynamics appear consistently.
Accommodation and enabling: partners adapt, generously and exhaustingly, taking over tasks, agreeing to separate arrangements, tiptoeing through mornings. These function as safety behaviors: short-term relief at the cost of long-term maintenance.
Role crystallization: one partner becomes the Identified Patient, the other the Helper or, eventually, the Impatient Bystander. In EFT terms, beneath the co-sleeper’s frustration lies almost always fear of lost intimacy, permanent damage, or helplessness. That secondary presentation drives the anxious partner deeper into shame and hypervigilance, sustaining the cycle.
Physical disconnection as relational loss: when couples stop sharing a bed, they frequently stop sharing other forms of closeness. The bed is not merely furniture. It is a relational space, and its loss carries relational meaning.
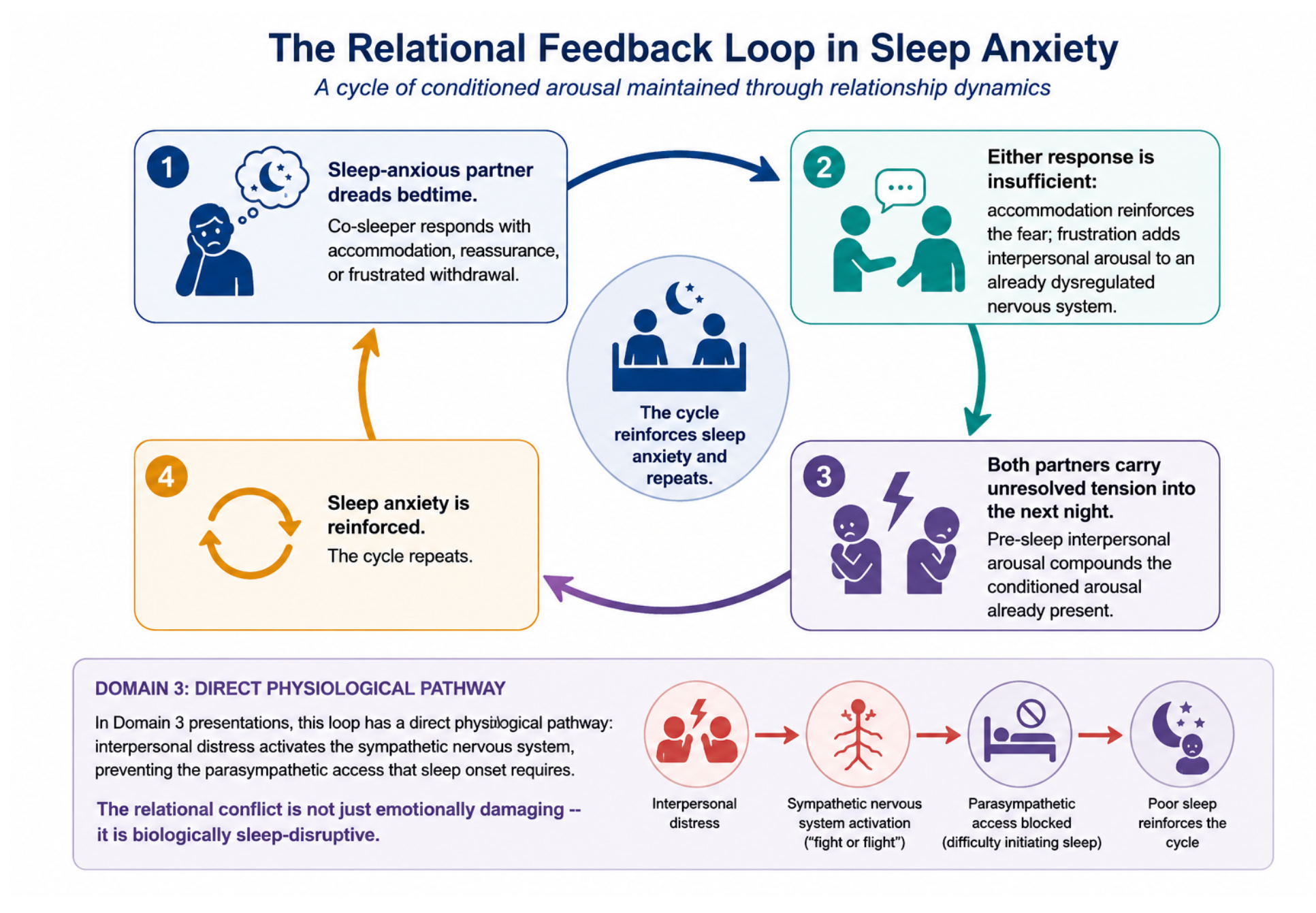
The figure below illustrates the recursive interpersonal processes through which sleep anxiety may become maintained within couple relationships. A sleep-anxious individual approaches bedtime with anticipatory fear and heightened arousal, prompting the co-sleeper to respond through reassurance, accommodation, problem-solving, or frustrated withdrawal. Although often well-intentioned, these responses may inadvertently reinforce anxiety or increase interpersonal tension, further amplifying pre-sleep arousal. Over time, unresolved relational stress and conditioned hypervigilance become linked to the sleep environment, perpetuating both insomnia and dyadic distress. The lower panel illustrates a Domain 3 pathway in which interpersonal conflict activates sympathetic nervous system arousal, interferes with parasympathetic downregulation necessary for sleep initiation, and contributes to the ongoing biological reinforcement of sleep disruption.
Assessment: Asking the right questions
Effective assessment requires two parallel tracks: identifying the domain of sleep anxiety, and mapping how the relational system has organized around it.
Identifying the domain. For fear of sleeplessness: What are you most afraid will happen if you don’t sleep? Do you monitor your body at bedtime for signs of sleepiness? Do you have rituals designed to guarantee sleep? For fear of sleep itself: Is there anything frightening about actually falling asleep, such as losing awareness, not knowing what’s happening around you? Have you had sleep paralysis or disturbing dreams that made you wary of sleep? For nighttime nervous system dysregulation: When you try to relax, does your anxiety increase? Have relaxation techniques ever seemed to make things worse?
Mapping the relational system. Do you share a sleep space? If not, how did that change come about? How does your partner respond when you have a bad night and how does that feel? What have each of you given up because of this?
These two tracks create the formulation. A Domain 1 client whose partner provides nightly reassurance requires a fundamentally different move than a Domain 3 client whose pre-sleep conflict is physiologically preventing the autonomic shift sleep onset requires.
Clinical interventions: What MFTs can do
None of the following require extensive behavioral sleep medicine training. They require willingness to see the sleep problem systemically.
Reframe the unit of treatment Make the relational architecture visible. Sleep anxiety in one partner is a problem in the couple system; both are involved in its maintenance, both have a role in its resolution. Naming the domain is part of the reframe; a clinically precise name is itself therapeutic:
“What you’re describing sounds less like a sleep problem and more like a fear problem that lives at the threshold of sleep. That’s a specific thing—and it’s something we can work on as a couple, because it clearly exists between you as much as it is inside either of you.”
Map and interrupt domain-specific accommodation. In Domain 1, shift the co-sleeper from reassurance to presence without problem-solving: not “You’ll be fine” but “I’m here. You don’t have to fix tonight.” Reassurance confirms threat; presence communicates safety. In Domain 2, interrupt environmental accommodations (lights left on, agreements to check in) that prevent a graduated approach to the feared stimulus; involve the co-sleeper as a safe companion in that reapproach, not a rescuer. In Domain 3, interrupt pre-sleep interpersonal conflict. A tense exchange before bed is not merely emotionally disruptive, it is physiologically disruptive for a nervous system already struggling to access parasympathetic states (Forman, 2026). A relational wind-down protocol is a neurobiological intervention.
Externalize the anxiety. Naming the anxiety as an entity that has moved into the bedroom allows the couple to face it together rather than face each other. Domain-specific language helps: “the Sleep Monitor” for Domain 1, “the Sentinel” for Domain 2, “the Alarm That Won’t Turn Off” for Domain 3. Couples find these framings accurate and relieving; they name something felt but unspoken.
Engage the attachment layer. Perceived partner responsiveness is among the strongest relational predictors of sleep quality (Troxel, 2010; Forman, in press). For Domain 2 clients, EFT-style attachment work—explicit conversations about what each partner needs to feel safe at night—functions as a direct sleep intervention (Johnson, 2019). For Domain 3 clients, the calm, regulated presence of a trusted attachment figure activates the ventral vagal circuit associated with safety, directly supporting the parasympathetic shift sleep onset requires (Porges, 2011). Co-regulation between partners is not a metaphor. It is physiology.
Offer domain-specific psychoeducation to both partners, in session, together. For Domain 1: sleep cannot be willed; effort is the enemy of sleep onset; monitoring and rituals are the maintaining mechanism, not the solution. For Domain 2: fear of sleep is a coherent clinical presentation with a treatment pathway, not a character flaw; sleep restriction is often contraindicated without prior fear-reduction work. For Domain 3: the relaxation paradox is real; prescribing relaxation without assessing for RIA will worsen the presentation. The co-sleeper who understands these distinctions stops offering remedies that don’t fit and starts providing the support their partner’s domain actually requires.
A note on sleeping apart
Separate sleeping arrangements almost never receive direct clinical attention and almost always deserve it. The decision accumulates one night at a time until it calcifies. The clinical question is not whether sleeping apart is right or wrong, but whether it is a thoughtful mutual decision or an anxious avoidance maintaining the very fear it was meant to manage. For Domain 1 clients, it reduces short-term pressure while reinforcing long-term avoidance. For Domain 2 clients, it may directly express the fear of vulnerability. For Domain 3 clients, it removes one of the most effective available resources: the co-regulatory presence of a calm and trusted partner.
The sleep is the relationship
The fear does not live in one partner’s nervous system in isolation. It lives in accommodation patterns, unspoken losses, and circular processes that sustain it across years of shared life. The relational system is part of the problem and, when engaged skillfully, part of the solution.
Jared and Shelly found their way back to a shared bedroom. He learned to stop prescribing remedies and start offering presence. She learned that her fear was a conditioned response with a name and a pathway out. They stopped sleeping together. Then they started understanding each other. The sleep came later, but it came, because the relationship could finally hold it.
MFTs don’t need to become sleep specialists to do this work. They need a clinical map, a willingness to ask the right questions, and confidence that the relational lens they bring to every other presenting problem is exactly the lens this one requires.
The following clinical summary translates the three-domain framework into practical intervention targets for MFTs. The guide is intended as a quick-reference tool for identifying the dominant presentation pattern, recognizing common relational maintenance processes, and selecting domain-specific therapeutic responses.
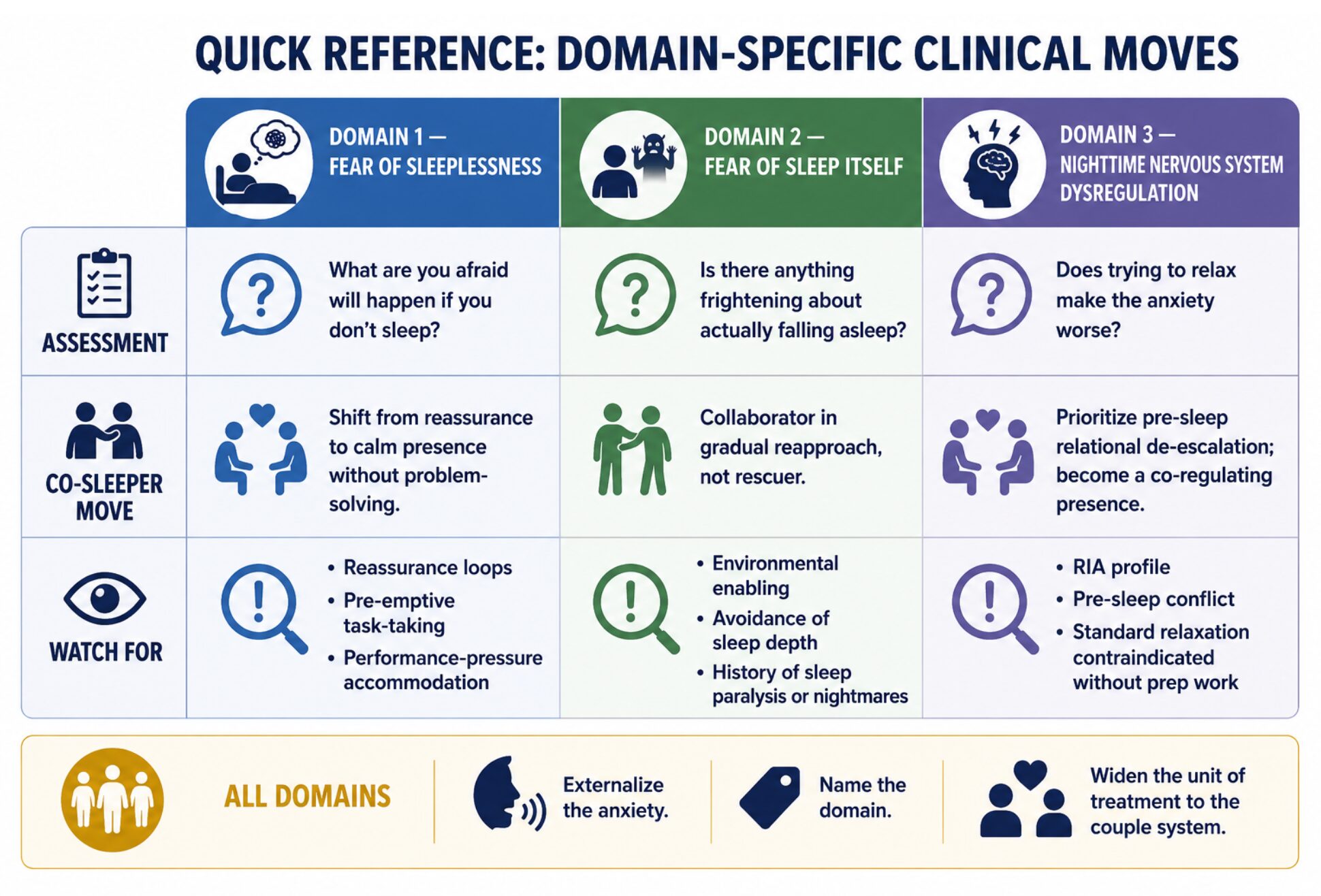
This figure provides a concise clinical framework for assessing and responding to the three major presentations of sleep anxiety within couple relationships. For each domain, the guide identifies core assessment questions, recommended co-sleeper responses, and common relational patterns that may inadvertently maintain insomnia-related fear and arousal. Across all domains, treatment emphasizes reducing accommodation, strengthening co-regulation, and approaching sleep anxiety as a relational rather than exclusively individual problem.

Bruce D. Forman, PhD, practices trauma-informed behavioral sleep medicine in Weston, Florida, via telehealth. He was previously director of MFT training in the Counseling Psychology program at the University of Miami and is a Professional member of AAMFT, joining in 1980. His latest book is titled For God’s Sake Go to Sleep: Insights About Sleep from Jewish Tradition & Modern Science.
Forman, B. D. (2026). Insomnia as a disorder of threat perception. Journal of Contemporary Psychotherapy. https://doi.org/10.1007/s10879-026-09725-w
Forman, B. D. (in preparation). The Multilevel architecture of sleep anxiety model (MASAM).
Forman, B. D. (in press). Couple- and family-based interventions for insomnia and OSA: A 25-year systematic review. Couple and Family Psychology: Research and Practice.
Hazlett-Stevens, H., & Craske, M. G. (2003). The catastrophizing worry process in generalized anxiety disorder. Cognitive Behaviour Therapy, 32(1), 44–52.
Johnson, S. M. (2019). Attachment theory in practice. Guilford Press.
Porges, S. W. (2011). The polyvagal theory. W. W. Norton.
Troxel, W. M. (2010). It’s more than sex. Psychosomatic Medicine, 72(6), 578–586.
Troxel, W. M., Robles, T. F., Hall, M., & Buysse, D. J. (2007). Marital quality and the marital bed. Sleep Medicine Reviews, 11(5), 389–404.
Other articles

Feature
Closing the Gap Between Knowing and Doing: AI Avatars in MFT Training
A graduate student begins a session with a couple. One partner does most of the talking. The other gives short, brief answers. Inside of two minutes, the talkative partner keeps pressing the student to take their side, and the student has to decide, right then, whether to follow their lead or turn toward the quieter partner.
Jay Burke, PsyD, & Sofia Georgiadou, PhD

Feature
The Space Between Us: A Systemic Approach to Relational Endings
Relational endings might be one of the experiences that can reveal the most vulnerable parts of ourselves—ruptured stories collapsed into an idea of what could have been. In our capacity as systemic practitioners, we get to listen to several stories of longing: romantic relationships that have dissolved without notice, friendships that no longer hold, family (dis)connections that can stretch across silence and distance.
Danna Abraham, PhD & Yuritzi Uribe Lemus, MA

Feature
Yours, Mine, and Ours: Helping Couples Organize Money
There is a question most therapists rarely think to ask, yet the answer can open the door to some of the most revealing clinical conversations: How do you and your partner actually organize your money?
John L. Hankins, MSS